- Privacy Policy
Home » Case Study – Methods, Examples and Guide

Case Study – Methods, Examples and Guide
Table of Contents

A case study is a research method that involves an in-depth examination and analysis of a particular phenomenon or case, such as an individual, organization, community, event, or situation.
It is a qualitative research approach that aims to provide a detailed and comprehensive understanding of the case being studied. Case studies typically involve multiple sources of data, including interviews, observations, documents, and artifacts, which are analyzed using various techniques, such as content analysis, thematic analysis, and grounded theory. The findings of a case study are often used to develop theories, inform policy or practice, or generate new research questions.
Types of Case Study
Types and Methods of Case Study are as follows:
Single-Case Study
A single-case study is an in-depth analysis of a single case. This type of case study is useful when the researcher wants to understand a specific phenomenon in detail.
For Example , A researcher might conduct a single-case study on a particular individual to understand their experiences with a particular health condition or a specific organization to explore their management practices. The researcher collects data from multiple sources, such as interviews, observations, and documents, and uses various techniques to analyze the data, such as content analysis or thematic analysis. The findings of a single-case study are often used to generate new research questions, develop theories, or inform policy or practice.
Multiple-Case Study
A multiple-case study involves the analysis of several cases that are similar in nature. This type of case study is useful when the researcher wants to identify similarities and differences between the cases.
For Example, a researcher might conduct a multiple-case study on several companies to explore the factors that contribute to their success or failure. The researcher collects data from each case, compares and contrasts the findings, and uses various techniques to analyze the data, such as comparative analysis or pattern-matching. The findings of a multiple-case study can be used to develop theories, inform policy or practice, or generate new research questions.
Exploratory Case Study
An exploratory case study is used to explore a new or understudied phenomenon. This type of case study is useful when the researcher wants to generate hypotheses or theories about the phenomenon.
For Example, a researcher might conduct an exploratory case study on a new technology to understand its potential impact on society. The researcher collects data from multiple sources, such as interviews, observations, and documents, and uses various techniques to analyze the data, such as grounded theory or content analysis. The findings of an exploratory case study can be used to generate new research questions, develop theories, or inform policy or practice.
Descriptive Case Study
A descriptive case study is used to describe a particular phenomenon in detail. This type of case study is useful when the researcher wants to provide a comprehensive account of the phenomenon.
For Example, a researcher might conduct a descriptive case study on a particular community to understand its social and economic characteristics. The researcher collects data from multiple sources, such as interviews, observations, and documents, and uses various techniques to analyze the data, such as content analysis or thematic analysis. The findings of a descriptive case study can be used to inform policy or practice or generate new research questions.
Instrumental Case Study
An instrumental case study is used to understand a particular phenomenon that is instrumental in achieving a particular goal. This type of case study is useful when the researcher wants to understand the role of the phenomenon in achieving the goal.
For Example, a researcher might conduct an instrumental case study on a particular policy to understand its impact on achieving a particular goal, such as reducing poverty. The researcher collects data from multiple sources, such as interviews, observations, and documents, and uses various techniques to analyze the data, such as content analysis or thematic analysis. The findings of an instrumental case study can be used to inform policy or practice or generate new research questions.
Case Study Data Collection Methods
Here are some common data collection methods for case studies:
Interviews involve asking questions to individuals who have knowledge or experience relevant to the case study. Interviews can be structured (where the same questions are asked to all participants) or unstructured (where the interviewer follows up on the responses with further questions). Interviews can be conducted in person, over the phone, or through video conferencing.
Observations
Observations involve watching and recording the behavior and activities of individuals or groups relevant to the case study. Observations can be participant (where the researcher actively participates in the activities) or non-participant (where the researcher observes from a distance). Observations can be recorded using notes, audio or video recordings, or photographs.
Documents can be used as a source of information for case studies. Documents can include reports, memos, emails, letters, and other written materials related to the case study. Documents can be collected from the case study participants or from public sources.
Surveys involve asking a set of questions to a sample of individuals relevant to the case study. Surveys can be administered in person, over the phone, through mail or email, or online. Surveys can be used to gather information on attitudes, opinions, or behaviors related to the case study.
Artifacts are physical objects relevant to the case study. Artifacts can include tools, equipment, products, or other objects that provide insights into the case study phenomenon.
How to conduct Case Study Research
Conducting a case study research involves several steps that need to be followed to ensure the quality and rigor of the study. Here are the steps to conduct case study research:
- Define the research questions: The first step in conducting a case study research is to define the research questions. The research questions should be specific, measurable, and relevant to the case study phenomenon under investigation.
- Select the case: The next step is to select the case or cases to be studied. The case should be relevant to the research questions and should provide rich and diverse data that can be used to answer the research questions.
- Collect data: Data can be collected using various methods, such as interviews, observations, documents, surveys, and artifacts. The data collection method should be selected based on the research questions and the nature of the case study phenomenon.
- Analyze the data: The data collected from the case study should be analyzed using various techniques, such as content analysis, thematic analysis, or grounded theory. The analysis should be guided by the research questions and should aim to provide insights and conclusions relevant to the research questions.
- Draw conclusions: The conclusions drawn from the case study should be based on the data analysis and should be relevant to the research questions. The conclusions should be supported by evidence and should be clearly stated.
- Validate the findings: The findings of the case study should be validated by reviewing the data and the analysis with participants or other experts in the field. This helps to ensure the validity and reliability of the findings.
- Write the report: The final step is to write the report of the case study research. The report should provide a clear description of the case study phenomenon, the research questions, the data collection methods, the data analysis, the findings, and the conclusions. The report should be written in a clear and concise manner and should follow the guidelines for academic writing.
Examples of Case Study
Here are some examples of case study research:
- The Hawthorne Studies : Conducted between 1924 and 1932, the Hawthorne Studies were a series of case studies conducted by Elton Mayo and his colleagues to examine the impact of work environment on employee productivity. The studies were conducted at the Hawthorne Works plant of the Western Electric Company in Chicago and included interviews, observations, and experiments.
- The Stanford Prison Experiment: Conducted in 1971, the Stanford Prison Experiment was a case study conducted by Philip Zimbardo to examine the psychological effects of power and authority. The study involved simulating a prison environment and assigning participants to the role of guards or prisoners. The study was controversial due to the ethical issues it raised.
- The Challenger Disaster: The Challenger Disaster was a case study conducted to examine the causes of the Space Shuttle Challenger explosion in 1986. The study included interviews, observations, and analysis of data to identify the technical, organizational, and cultural factors that contributed to the disaster.
- The Enron Scandal: The Enron Scandal was a case study conducted to examine the causes of the Enron Corporation’s bankruptcy in 2001. The study included interviews, analysis of financial data, and review of documents to identify the accounting practices, corporate culture, and ethical issues that led to the company’s downfall.
- The Fukushima Nuclear Disaster : The Fukushima Nuclear Disaster was a case study conducted to examine the causes of the nuclear accident that occurred at the Fukushima Daiichi Nuclear Power Plant in Japan in 2011. The study included interviews, analysis of data, and review of documents to identify the technical, organizational, and cultural factors that contributed to the disaster.
Application of Case Study
Case studies have a wide range of applications across various fields and industries. Here are some examples:
Business and Management
Case studies are widely used in business and management to examine real-life situations and develop problem-solving skills. Case studies can help students and professionals to develop a deep understanding of business concepts, theories, and best practices.
Case studies are used in healthcare to examine patient care, treatment options, and outcomes. Case studies can help healthcare professionals to develop critical thinking skills, diagnose complex medical conditions, and develop effective treatment plans.
Case studies are used in education to examine teaching and learning practices. Case studies can help educators to develop effective teaching strategies, evaluate student progress, and identify areas for improvement.
Social Sciences
Case studies are widely used in social sciences to examine human behavior, social phenomena, and cultural practices. Case studies can help researchers to develop theories, test hypotheses, and gain insights into complex social issues.
Law and Ethics
Case studies are used in law and ethics to examine legal and ethical dilemmas. Case studies can help lawyers, policymakers, and ethical professionals to develop critical thinking skills, analyze complex cases, and make informed decisions.
Purpose of Case Study
The purpose of a case study is to provide a detailed analysis of a specific phenomenon, issue, or problem in its real-life context. A case study is a qualitative research method that involves the in-depth exploration and analysis of a particular case, which can be an individual, group, organization, event, or community.
The primary purpose of a case study is to generate a comprehensive and nuanced understanding of the case, including its history, context, and dynamics. Case studies can help researchers to identify and examine the underlying factors, processes, and mechanisms that contribute to the case and its outcomes. This can help to develop a more accurate and detailed understanding of the case, which can inform future research, practice, or policy.
Case studies can also serve other purposes, including:
- Illustrating a theory or concept: Case studies can be used to illustrate and explain theoretical concepts and frameworks, providing concrete examples of how they can be applied in real-life situations.
- Developing hypotheses: Case studies can help to generate hypotheses about the causal relationships between different factors and outcomes, which can be tested through further research.
- Providing insight into complex issues: Case studies can provide insights into complex and multifaceted issues, which may be difficult to understand through other research methods.
- Informing practice or policy: Case studies can be used to inform practice or policy by identifying best practices, lessons learned, or areas for improvement.
Advantages of Case Study Research
There are several advantages of case study research, including:
- In-depth exploration: Case study research allows for a detailed exploration and analysis of a specific phenomenon, issue, or problem in its real-life context. This can provide a comprehensive understanding of the case and its dynamics, which may not be possible through other research methods.
- Rich data: Case study research can generate rich and detailed data, including qualitative data such as interviews, observations, and documents. This can provide a nuanced understanding of the case and its complexity.
- Holistic perspective: Case study research allows for a holistic perspective of the case, taking into account the various factors, processes, and mechanisms that contribute to the case and its outcomes. This can help to develop a more accurate and comprehensive understanding of the case.
- Theory development: Case study research can help to develop and refine theories and concepts by providing empirical evidence and concrete examples of how they can be applied in real-life situations.
- Practical application: Case study research can inform practice or policy by identifying best practices, lessons learned, or areas for improvement.
- Contextualization: Case study research takes into account the specific context in which the case is situated, which can help to understand how the case is influenced by the social, cultural, and historical factors of its environment.
Limitations of Case Study Research
There are several limitations of case study research, including:
- Limited generalizability : Case studies are typically focused on a single case or a small number of cases, which limits the generalizability of the findings. The unique characteristics of the case may not be applicable to other contexts or populations, which may limit the external validity of the research.
- Biased sampling: Case studies may rely on purposive or convenience sampling, which can introduce bias into the sample selection process. This may limit the representativeness of the sample and the generalizability of the findings.
- Subjectivity: Case studies rely on the interpretation of the researcher, which can introduce subjectivity into the analysis. The researcher’s own biases, assumptions, and perspectives may influence the findings, which may limit the objectivity of the research.
- Limited control: Case studies are typically conducted in naturalistic settings, which limits the control that the researcher has over the environment and the variables being studied. This may limit the ability to establish causal relationships between variables.
- Time-consuming: Case studies can be time-consuming to conduct, as they typically involve a detailed exploration and analysis of a specific case. This may limit the feasibility of conducting multiple case studies or conducting case studies in a timely manner.
- Resource-intensive: Case studies may require significant resources, including time, funding, and expertise. This may limit the ability of researchers to conduct case studies in resource-constrained settings.
About the author

Muhammad Hassan
Researcher, Academic Writer, Web developer
You may also like

Research Methods – Types, Examples and Guide

One-to-One Interview – Methods and Guide

Observational Research – Methods and Guide

Experimental Design – Types, Methods, Guide

Ethnographic Research -Types, Methods and Guide

Qualitative Research – Methods, Analysis Types...
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, generate accurate citations for free.
- Knowledge Base
Methodology
- What Is a Case Study? | Definition, Examples & Methods
What Is a Case Study? | Definition, Examples & Methods
Published on May 8, 2019 by Shona McCombes . Revised on November 20, 2023.
A case study is a detailed study of a specific subject, such as a person, group, place, event, organization, or phenomenon. Case studies are commonly used in social, educational, clinical, and business research.
A case study research design usually involves qualitative methods , but quantitative methods are sometimes also used. Case studies are good for describing , comparing, evaluating and understanding different aspects of a research problem .
Table of contents
When to do a case study, step 1: select a case, step 2: build a theoretical framework, step 3: collect your data, step 4: describe and analyze the case, other interesting articles.
A case study is an appropriate research design when you want to gain concrete, contextual, in-depth knowledge about a specific real-world subject. It allows you to explore the key characteristics, meanings, and implications of the case.
Case studies are often a good choice in a thesis or dissertation . They keep your project focused and manageable when you don’t have the time or resources to do large-scale research.
You might use just one complex case study where you explore a single subject in depth, or conduct multiple case studies to compare and illuminate different aspects of your research problem.
| Research question | Case study |
|---|---|
| What are the ecological effects of wolf reintroduction? | Case study of wolf reintroduction in Yellowstone National Park |
| How do populist politicians use narratives about history to gain support? | Case studies of Hungarian prime minister Viktor Orbán and US president Donald Trump |
| How can teachers implement active learning strategies in mixed-level classrooms? | Case study of a local school that promotes active learning |
| What are the main advantages and disadvantages of wind farms for rural communities? | Case studies of three rural wind farm development projects in different parts of the country |
| How are viral marketing strategies changing the relationship between companies and consumers? | Case study of the iPhone X marketing campaign |
| How do experiences of work in the gig economy differ by gender, race and age? | Case studies of Deliveroo and Uber drivers in London |
Here's why students love Scribbr's proofreading services
Discover proofreading & editing
Once you have developed your problem statement and research questions , you should be ready to choose the specific case that you want to focus on. A good case study should have the potential to:
- Provide new or unexpected insights into the subject
- Challenge or complicate existing assumptions and theories
- Propose practical courses of action to resolve a problem
- Open up new directions for future research
TipIf your research is more practical in nature and aims to simultaneously investigate an issue as you solve it, consider conducting action research instead.
Unlike quantitative or experimental research , a strong case study does not require a random or representative sample. In fact, case studies often deliberately focus on unusual, neglected, or outlying cases which may shed new light on the research problem.
Example of an outlying case studyIn the 1960s the town of Roseto, Pennsylvania was discovered to have extremely low rates of heart disease compared to the US average. It became an important case study for understanding previously neglected causes of heart disease.
However, you can also choose a more common or representative case to exemplify a particular category, experience or phenomenon.
Example of a representative case studyIn the 1920s, two sociologists used Muncie, Indiana as a case study of a typical American city that supposedly exemplified the changing culture of the US at the time.
While case studies focus more on concrete details than general theories, they should usually have some connection with theory in the field. This way the case study is not just an isolated description, but is integrated into existing knowledge about the topic. It might aim to:
- Exemplify a theory by showing how it explains the case under investigation
- Expand on a theory by uncovering new concepts and ideas that need to be incorporated
- Challenge a theory by exploring an outlier case that doesn’t fit with established assumptions
To ensure that your analysis of the case has a solid academic grounding, you should conduct a literature review of sources related to the topic and develop a theoretical framework . This means identifying key concepts and theories to guide your analysis and interpretation.
There are many different research methods you can use to collect data on your subject. Case studies tend to focus on qualitative data using methods such as interviews , observations , and analysis of primary and secondary sources (e.g., newspaper articles, photographs, official records). Sometimes a case study will also collect quantitative data.
Example of a mixed methods case studyFor a case study of a wind farm development in a rural area, you could collect quantitative data on employment rates and business revenue, collect qualitative data on local people’s perceptions and experiences, and analyze local and national media coverage of the development.
The aim is to gain as thorough an understanding as possible of the case and its context.
Receive feedback on language, structure, and formatting
Professional editors proofread and edit your paper by focusing on:
- Academic style
- Vague sentences
- Style consistency
See an example

In writing up the case study, you need to bring together all the relevant aspects to give as complete a picture as possible of the subject.
How you report your findings depends on the type of research you are doing. Some case studies are structured like a standard scientific paper or thesis , with separate sections or chapters for the methods , results and discussion .
Others are written in a more narrative style, aiming to explore the case from various angles and analyze its meanings and implications (for example, by using textual analysis or discourse analysis ).
In all cases, though, make sure to give contextual details about the case, connect it back to the literature and theory, and discuss how it fits into wider patterns or debates.
If you want to know more about statistics , methodology , or research bias , make sure to check out some of our other articles with explanations and examples.
- Normal distribution
- Degrees of freedom
- Null hypothesis
- Discourse analysis
- Control groups
- Mixed methods research
- Non-probability sampling
- Quantitative research
- Ecological validity
Research bias
- Rosenthal effect
- Implicit bias
- Cognitive bias
- Selection bias
- Negativity bias
- Status quo bias
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the “Cite this Scribbr article” button to automatically add the citation to our free Citation Generator.
McCombes, S. (2023, November 20). What Is a Case Study? | Definition, Examples & Methods. Scribbr. Retrieved September 18, 2024, from https://www.scribbr.com/methodology/case-study/
Is this article helpful?

Shona McCombes
Other students also liked, primary vs. secondary sources | difference & examples, what is a theoretical framework | guide to organizing, what is action research | definition & examples, get unlimited documents corrected.
✔ Free APA citation check included ✔ Unlimited document corrections ✔ Specialized in correcting academic texts
- Open access
- Published: 27 June 2011
The case study approach
- Sarah Crowe 1 ,
- Kathrin Cresswell 2 ,
- Ann Robertson 2 ,
- Guro Huby 3 ,
- Anthony Avery 1 &
- Aziz Sheikh 2
BMC Medical Research Methodology volume 11 , Article number: 100 ( 2011 ) Cite this article
798k Accesses
1122 Citations
43 Altmetric
Metrics details
The case study approach allows in-depth, multi-faceted explorations of complex issues in their real-life settings. The value of the case study approach is well recognised in the fields of business, law and policy, but somewhat less so in health services research. Based on our experiences of conducting several health-related case studies, we reflect on the different types of case study design, the specific research questions this approach can help answer, the data sources that tend to be used, and the particular advantages and disadvantages of employing this methodological approach. The paper concludes with key pointers to aid those designing and appraising proposals for conducting case study research, and a checklist to help readers assess the quality of case study reports.
Peer Review reports
Introduction
The case study approach is particularly useful to employ when there is a need to obtain an in-depth appreciation of an issue, event or phenomenon of interest, in its natural real-life context. Our aim in writing this piece is to provide insights into when to consider employing this approach and an overview of key methodological considerations in relation to the design, planning, analysis, interpretation and reporting of case studies.
The illustrative 'grand round', 'case report' and 'case series' have a long tradition in clinical practice and research. Presenting detailed critiques, typically of one or more patients, aims to provide insights into aspects of the clinical case and, in doing so, illustrate broader lessons that may be learnt. In research, the conceptually-related case study approach can be used, for example, to describe in detail a patient's episode of care, explore professional attitudes to and experiences of a new policy initiative or service development or more generally to 'investigate contemporary phenomena within its real-life context' [ 1 ]. Based on our experiences of conducting a range of case studies, we reflect on when to consider using this approach, discuss the key steps involved and illustrate, with examples, some of the practical challenges of attaining an in-depth understanding of a 'case' as an integrated whole. In keeping with previously published work, we acknowledge the importance of theory to underpin the design, selection, conduct and interpretation of case studies[ 2 ]. In so doing, we make passing reference to the different epistemological approaches used in case study research by key theoreticians and methodologists in this field of enquiry.
This paper is structured around the following main questions: What is a case study? What are case studies used for? How are case studies conducted? What are the potential pitfalls and how can these be avoided? We draw in particular on four of our own recently published examples of case studies (see Tables 1 , 2 , 3 and 4 ) and those of others to illustrate our discussion[ 3 – 7 ].
What is a case study?
A case study is a research approach that is used to generate an in-depth, multi-faceted understanding of a complex issue in its real-life context. It is an established research design that is used extensively in a wide variety of disciplines, particularly in the social sciences. A case study can be defined in a variety of ways (Table 5 ), the central tenet being the need to explore an event or phenomenon in depth and in its natural context. It is for this reason sometimes referred to as a "naturalistic" design; this is in contrast to an "experimental" design (such as a randomised controlled trial) in which the investigator seeks to exert control over and manipulate the variable(s) of interest.
Stake's work has been particularly influential in defining the case study approach to scientific enquiry. He has helpfully characterised three main types of case study: intrinsic , instrumental and collective [ 8 ]. An intrinsic case study is typically undertaken to learn about a unique phenomenon. The researcher should define the uniqueness of the phenomenon, which distinguishes it from all others. In contrast, the instrumental case study uses a particular case (some of which may be better than others) to gain a broader appreciation of an issue or phenomenon. The collective case study involves studying multiple cases simultaneously or sequentially in an attempt to generate a still broader appreciation of a particular issue.
These are however not necessarily mutually exclusive categories. In the first of our examples (Table 1 ), we undertook an intrinsic case study to investigate the issue of recruitment of minority ethnic people into the specific context of asthma research studies, but it developed into a instrumental case study through seeking to understand the issue of recruitment of these marginalised populations more generally, generating a number of the findings that are potentially transferable to other disease contexts[ 3 ]. In contrast, the other three examples (see Tables 2 , 3 and 4 ) employed collective case study designs to study the introduction of workforce reconfiguration in primary care, the implementation of electronic health records into hospitals, and to understand the ways in which healthcare students learn about patient safety considerations[ 4 – 6 ]. Although our study focusing on the introduction of General Practitioners with Specialist Interests (Table 2 ) was explicitly collective in design (four contrasting primary care organisations were studied), is was also instrumental in that this particular professional group was studied as an exemplar of the more general phenomenon of workforce redesign[ 4 ].
What are case studies used for?
According to Yin, case studies can be used to explain, describe or explore events or phenomena in the everyday contexts in which they occur[ 1 ]. These can, for example, help to understand and explain causal links and pathways resulting from a new policy initiative or service development (see Tables 2 and 3 , for example)[ 1 ]. In contrast to experimental designs, which seek to test a specific hypothesis through deliberately manipulating the environment (like, for example, in a randomised controlled trial giving a new drug to randomly selected individuals and then comparing outcomes with controls),[ 9 ] the case study approach lends itself well to capturing information on more explanatory ' how ', 'what' and ' why ' questions, such as ' how is the intervention being implemented and received on the ground?'. The case study approach can offer additional insights into what gaps exist in its delivery or why one implementation strategy might be chosen over another. This in turn can help develop or refine theory, as shown in our study of the teaching of patient safety in undergraduate curricula (Table 4 )[ 6 , 10 ]. Key questions to consider when selecting the most appropriate study design are whether it is desirable or indeed possible to undertake a formal experimental investigation in which individuals and/or organisations are allocated to an intervention or control arm? Or whether the wish is to obtain a more naturalistic understanding of an issue? The former is ideally studied using a controlled experimental design, whereas the latter is more appropriately studied using a case study design.
Case studies may be approached in different ways depending on the epistemological standpoint of the researcher, that is, whether they take a critical (questioning one's own and others' assumptions), interpretivist (trying to understand individual and shared social meanings) or positivist approach (orientating towards the criteria of natural sciences, such as focusing on generalisability considerations) (Table 6 ). Whilst such a schema can be conceptually helpful, it may be appropriate to draw on more than one approach in any case study, particularly in the context of conducting health services research. Doolin has, for example, noted that in the context of undertaking interpretative case studies, researchers can usefully draw on a critical, reflective perspective which seeks to take into account the wider social and political environment that has shaped the case[ 11 ].
How are case studies conducted?
Here, we focus on the main stages of research activity when planning and undertaking a case study; the crucial stages are: defining the case; selecting the case(s); collecting and analysing the data; interpreting data; and reporting the findings.
Defining the case
Carefully formulated research question(s), informed by the existing literature and a prior appreciation of the theoretical issues and setting(s), are all important in appropriately and succinctly defining the case[ 8 , 12 ]. Crucially, each case should have a pre-defined boundary which clarifies the nature and time period covered by the case study (i.e. its scope, beginning and end), the relevant social group, organisation or geographical area of interest to the investigator, the types of evidence to be collected, and the priorities for data collection and analysis (see Table 7 )[ 1 ]. A theory driven approach to defining the case may help generate knowledge that is potentially transferable to a range of clinical contexts and behaviours; using theory is also likely to result in a more informed appreciation of, for example, how and why interventions have succeeded or failed[ 13 ].
For example, in our evaluation of the introduction of electronic health records in English hospitals (Table 3 ), we defined our cases as the NHS Trusts that were receiving the new technology[ 5 ]. Our focus was on how the technology was being implemented. However, if the primary research interest had been on the social and organisational dimensions of implementation, we might have defined our case differently as a grouping of healthcare professionals (e.g. doctors and/or nurses). The precise beginning and end of the case may however prove difficult to define. Pursuing this same example, when does the process of implementation and adoption of an electronic health record system really begin or end? Such judgements will inevitably be influenced by a range of factors, including the research question, theory of interest, the scope and richness of the gathered data and the resources available to the research team.
Selecting the case(s)
The decision on how to select the case(s) to study is a very important one that merits some reflection. In an intrinsic case study, the case is selected on its own merits[ 8 ]. The case is selected not because it is representative of other cases, but because of its uniqueness, which is of genuine interest to the researchers. This was, for example, the case in our study of the recruitment of minority ethnic participants into asthma research (Table 1 ) as our earlier work had demonstrated the marginalisation of minority ethnic people with asthma, despite evidence of disproportionate asthma morbidity[ 14 , 15 ]. In another example of an intrinsic case study, Hellstrom et al.[ 16 ] studied an elderly married couple living with dementia to explore how dementia had impacted on their understanding of home, their everyday life and their relationships.
For an instrumental case study, selecting a "typical" case can work well[ 8 ]. In contrast to the intrinsic case study, the particular case which is chosen is of less importance than selecting a case that allows the researcher to investigate an issue or phenomenon. For example, in order to gain an understanding of doctors' responses to health policy initiatives, Som undertook an instrumental case study interviewing clinicians who had a range of responsibilities for clinical governance in one NHS acute hospital trust[ 17 ]. Sampling a "deviant" or "atypical" case may however prove even more informative, potentially enabling the researcher to identify causal processes, generate hypotheses and develop theory.
In collective or multiple case studies, a number of cases are carefully selected. This offers the advantage of allowing comparisons to be made across several cases and/or replication. Choosing a "typical" case may enable the findings to be generalised to theory (i.e. analytical generalisation) or to test theory by replicating the findings in a second or even a third case (i.e. replication logic)[ 1 ]. Yin suggests two or three literal replications (i.e. predicting similar results) if the theory is straightforward and five or more if the theory is more subtle. However, critics might argue that selecting 'cases' in this way is insufficiently reflexive and ill-suited to the complexities of contemporary healthcare organisations.
The selected case study site(s) should allow the research team access to the group of individuals, the organisation, the processes or whatever else constitutes the chosen unit of analysis for the study. Access is therefore a central consideration; the researcher needs to come to know the case study site(s) well and to work cooperatively with them. Selected cases need to be not only interesting but also hospitable to the inquiry [ 8 ] if they are to be informative and answer the research question(s). Case study sites may also be pre-selected for the researcher, with decisions being influenced by key stakeholders. For example, our selection of case study sites in the evaluation of the implementation and adoption of electronic health record systems (see Table 3 ) was heavily influenced by NHS Connecting for Health, the government agency that was responsible for overseeing the National Programme for Information Technology (NPfIT)[ 5 ]. This prominent stakeholder had already selected the NHS sites (through a competitive bidding process) to be early adopters of the electronic health record systems and had negotiated contracts that detailed the deployment timelines.
It is also important to consider in advance the likely burden and risks associated with participation for those who (or the site(s) which) comprise the case study. Of particular importance is the obligation for the researcher to think through the ethical implications of the study (e.g. the risk of inadvertently breaching anonymity or confidentiality) and to ensure that potential participants/participating sites are provided with sufficient information to make an informed choice about joining the study. The outcome of providing this information might be that the emotive burden associated with participation, or the organisational disruption associated with supporting the fieldwork, is considered so high that the individuals or sites decide against participation.
In our example of evaluating implementations of electronic health record systems, given the restricted number of early adopter sites available to us, we sought purposively to select a diverse range of implementation cases among those that were available[ 5 ]. We chose a mixture of teaching, non-teaching and Foundation Trust hospitals, and examples of each of the three electronic health record systems procured centrally by the NPfIT. At one recruited site, it quickly became apparent that access was problematic because of competing demands on that organisation. Recognising the importance of full access and co-operative working for generating rich data, the research team decided not to pursue work at that site and instead to focus on other recruited sites.
Collecting the data
In order to develop a thorough understanding of the case, the case study approach usually involves the collection of multiple sources of evidence, using a range of quantitative (e.g. questionnaires, audits and analysis of routinely collected healthcare data) and more commonly qualitative techniques (e.g. interviews, focus groups and observations). The use of multiple sources of data (data triangulation) has been advocated as a way of increasing the internal validity of a study (i.e. the extent to which the method is appropriate to answer the research question)[ 8 , 18 – 21 ]. An underlying assumption is that data collected in different ways should lead to similar conclusions, and approaching the same issue from different angles can help develop a holistic picture of the phenomenon (Table 2 )[ 4 ].
Brazier and colleagues used a mixed-methods case study approach to investigate the impact of a cancer care programme[ 22 ]. Here, quantitative measures were collected with questionnaires before, and five months after, the start of the intervention which did not yield any statistically significant results. Qualitative interviews with patients however helped provide an insight into potentially beneficial process-related aspects of the programme, such as greater, perceived patient involvement in care. The authors reported how this case study approach provided a number of contextual factors likely to influence the effectiveness of the intervention and which were not likely to have been obtained from quantitative methods alone.
In collective or multiple case studies, data collection needs to be flexible enough to allow a detailed description of each individual case to be developed (e.g. the nature of different cancer care programmes), before considering the emerging similarities and differences in cross-case comparisons (e.g. to explore why one programme is more effective than another). It is important that data sources from different cases are, where possible, broadly comparable for this purpose even though they may vary in nature and depth.
Analysing, interpreting and reporting case studies
Making sense and offering a coherent interpretation of the typically disparate sources of data (whether qualitative alone or together with quantitative) is far from straightforward. Repeated reviewing and sorting of the voluminous and detail-rich data are integral to the process of analysis. In collective case studies, it is helpful to analyse data relating to the individual component cases first, before making comparisons across cases. Attention needs to be paid to variations within each case and, where relevant, the relationship between different causes, effects and outcomes[ 23 ]. Data will need to be organised and coded to allow the key issues, both derived from the literature and emerging from the dataset, to be easily retrieved at a later stage. An initial coding frame can help capture these issues and can be applied systematically to the whole dataset with the aid of a qualitative data analysis software package.
The Framework approach is a practical approach, comprising of five stages (familiarisation; identifying a thematic framework; indexing; charting; mapping and interpretation) , to managing and analysing large datasets particularly if time is limited, as was the case in our study of recruitment of South Asians into asthma research (Table 1 )[ 3 , 24 ]. Theoretical frameworks may also play an important role in integrating different sources of data and examining emerging themes. For example, we drew on a socio-technical framework to help explain the connections between different elements - technology; people; and the organisational settings within which they worked - in our study of the introduction of electronic health record systems (Table 3 )[ 5 ]. Our study of patient safety in undergraduate curricula drew on an evaluation-based approach to design and analysis, which emphasised the importance of the academic, organisational and practice contexts through which students learn (Table 4 )[ 6 ].
Case study findings can have implications both for theory development and theory testing. They may establish, strengthen or weaken historical explanations of a case and, in certain circumstances, allow theoretical (as opposed to statistical) generalisation beyond the particular cases studied[ 12 ]. These theoretical lenses should not, however, constitute a strait-jacket and the cases should not be "forced to fit" the particular theoretical framework that is being employed.
When reporting findings, it is important to provide the reader with enough contextual information to understand the processes that were followed and how the conclusions were reached. In a collective case study, researchers may choose to present the findings from individual cases separately before amalgamating across cases. Care must be taken to ensure the anonymity of both case sites and individual participants (if agreed in advance) by allocating appropriate codes or withholding descriptors. In the example given in Table 3 , we decided against providing detailed information on the NHS sites and individual participants in order to avoid the risk of inadvertent disclosure of identities[ 5 , 25 ].
What are the potential pitfalls and how can these be avoided?
The case study approach is, as with all research, not without its limitations. When investigating the formal and informal ways undergraduate students learn about patient safety (Table 4 ), for example, we rapidly accumulated a large quantity of data. The volume of data, together with the time restrictions in place, impacted on the depth of analysis that was possible within the available resources. This highlights a more general point of the importance of avoiding the temptation to collect as much data as possible; adequate time also needs to be set aside for data analysis and interpretation of what are often highly complex datasets.
Case study research has sometimes been criticised for lacking scientific rigour and providing little basis for generalisation (i.e. producing findings that may be transferable to other settings)[ 1 ]. There are several ways to address these concerns, including: the use of theoretical sampling (i.e. drawing on a particular conceptual framework); respondent validation (i.e. participants checking emerging findings and the researcher's interpretation, and providing an opinion as to whether they feel these are accurate); and transparency throughout the research process (see Table 8 )[ 8 , 18 – 21 , 23 , 26 ]. Transparency can be achieved by describing in detail the steps involved in case selection, data collection, the reasons for the particular methods chosen, and the researcher's background and level of involvement (i.e. being explicit about how the researcher has influenced data collection and interpretation). Seeking potential, alternative explanations, and being explicit about how interpretations and conclusions were reached, help readers to judge the trustworthiness of the case study report. Stake provides a critique checklist for a case study report (Table 9 )[ 8 ].
Conclusions
The case study approach allows, amongst other things, critical events, interventions, policy developments and programme-based service reforms to be studied in detail in a real-life context. It should therefore be considered when an experimental design is either inappropriate to answer the research questions posed or impossible to undertake. Considering the frequency with which implementations of innovations are now taking place in healthcare settings and how well the case study approach lends itself to in-depth, complex health service research, we believe this approach should be more widely considered by researchers. Though inherently challenging, the research case study can, if carefully conceptualised and thoughtfully undertaken and reported, yield powerful insights into many important aspects of health and healthcare delivery.
Yin RK: Case study research, design and method. 2009, London: Sage Publications Ltd., 4
Google Scholar
Keen J, Packwood T: Qualitative research; case study evaluation. BMJ. 1995, 311: 444-446.
Article CAS PubMed PubMed Central Google Scholar
Sheikh A, Halani L, Bhopal R, Netuveli G, Partridge M, Car J, et al: Facilitating the Recruitment of Minority Ethnic People into Research: Qualitative Case Study of South Asians and Asthma. PLoS Med. 2009, 6 (10): 1-11.
Article Google Scholar
Pinnock H, Huby G, Powell A, Kielmann T, Price D, Williams S, et al: The process of planning, development and implementation of a General Practitioner with a Special Interest service in Primary Care Organisations in England and Wales: a comparative prospective case study. Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R&D (NCCSDO). 2008, [ http://www.sdo.nihr.ac.uk/files/project/99-final-report.pdf ]
Robertson A, Cresswell K, Takian A, Petrakaki D, Crowe S, Cornford T, et al: Prospective evaluation of the implementation and adoption of NHS Connecting for Health's national electronic health record in secondary care in England: interim findings. BMJ. 2010, 41: c4564-
Pearson P, Steven A, Howe A, Sheikh A, Ashcroft D, Smith P, the Patient Safety Education Study Group: Learning about patient safety: organisational context and culture in the education of healthcare professionals. J Health Serv Res Policy. 2010, 15: 4-10. 10.1258/jhsrp.2009.009052.
Article PubMed Google Scholar
van Harten WH, Casparie TF, Fisscher OA: The evaluation of the introduction of a quality management system: a process-oriented case study in a large rehabilitation hospital. Health Policy. 2002, 60 (1): 17-37. 10.1016/S0168-8510(01)00187-7.
Stake RE: The art of case study research. 1995, London: Sage Publications Ltd.
Sheikh A, Smeeth L, Ashcroft R: Randomised controlled trials in primary care: scope and application. Br J Gen Pract. 2002, 52 (482): 746-51.
PubMed PubMed Central Google Scholar
King G, Keohane R, Verba S: Designing Social Inquiry. 1996, Princeton: Princeton University Press
Doolin B: Information technology as disciplinary technology: being critical in interpretative research on information systems. Journal of Information Technology. 1998, 13: 301-311. 10.1057/jit.1998.8.
George AL, Bennett A: Case studies and theory development in the social sciences. 2005, Cambridge, MA: MIT Press
Eccles M, the Improved Clinical Effectiveness through Behavioural Research Group (ICEBeRG): Designing theoretically-informed implementation interventions. Implementation Science. 2006, 1: 1-8. 10.1186/1748-5908-1-1.
Article PubMed Central Google Scholar
Netuveli G, Hurwitz B, Levy M, Fletcher M, Barnes G, Durham SR, Sheikh A: Ethnic variations in UK asthma frequency, morbidity, and health-service use: a systematic review and meta-analysis. Lancet. 2005, 365 (9456): 312-7.
Sheikh A, Panesar SS, Lasserson T, Netuveli G: Recruitment of ethnic minorities to asthma studies. Thorax. 2004, 59 (7): 634-
CAS PubMed PubMed Central Google Scholar
Hellström I, Nolan M, Lundh U: 'We do things together': A case study of 'couplehood' in dementia. Dementia. 2005, 4: 7-22. 10.1177/1471301205049188.
Som CV: Nothing seems to have changed, nothing seems to be changing and perhaps nothing will change in the NHS: doctors' response to clinical governance. International Journal of Public Sector Management. 2005, 18: 463-477. 10.1108/09513550510608903.
Lincoln Y, Guba E: Naturalistic inquiry. 1985, Newbury Park: Sage Publications
Barbour RS: Checklists for improving rigour in qualitative research: a case of the tail wagging the dog?. BMJ. 2001, 322: 1115-1117. 10.1136/bmj.322.7294.1115.
Mays N, Pope C: Qualitative research in health care: Assessing quality in qualitative research. BMJ. 2000, 320: 50-52. 10.1136/bmj.320.7226.50.
Mason J: Qualitative researching. 2002, London: Sage
Brazier A, Cooke K, Moravan V: Using Mixed Methods for Evaluating an Integrative Approach to Cancer Care: A Case Study. Integr Cancer Ther. 2008, 7: 5-17. 10.1177/1534735407313395.
Miles MB, Huberman M: Qualitative data analysis: an expanded sourcebook. 1994, CA: Sage Publications Inc., 2
Pope C, Ziebland S, Mays N: Analysing qualitative data. Qualitative research in health care. BMJ. 2000, 320: 114-116. 10.1136/bmj.320.7227.114.
Cresswell KM, Worth A, Sheikh A: Actor-Network Theory and its role in understanding the implementation of information technology developments in healthcare. BMC Med Inform Decis Mak. 2010, 10 (1): 67-10.1186/1472-6947-10-67.
Article PubMed PubMed Central Google Scholar
Malterud K: Qualitative research: standards, challenges, and guidelines. Lancet. 2001, 358: 483-488. 10.1016/S0140-6736(01)05627-6.
Article CAS PubMed Google Scholar
Yin R: Case study research: design and methods. 1994, Thousand Oaks, CA: Sage Publishing, 2
Yin R: Enhancing the quality of case studies in health services research. Health Serv Res. 1999, 34: 1209-1224.
Green J, Thorogood N: Qualitative methods for health research. 2009, Los Angeles: Sage, 2
Howcroft D, Trauth E: Handbook of Critical Information Systems Research, Theory and Application. 2005, Cheltenham, UK: Northampton, MA, USA: Edward Elgar
Book Google Scholar
Blakie N: Approaches to Social Enquiry. 1993, Cambridge: Polity Press
Doolin B: Power and resistance in the implementation of a medical management information system. Info Systems J. 2004, 14: 343-362. 10.1111/j.1365-2575.2004.00176.x.
Bloomfield BP, Best A: Management consultants: systems development, power and the translation of problems. Sociological Review. 1992, 40: 533-560.
Shanks G, Parr A: Positivist, single case study research in information systems: A critical analysis. Proceedings of the European Conference on Information Systems. 2003, Naples
Pre-publication history
The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1471-2288/11/100/prepub
Download references
Acknowledgements
We are grateful to the participants and colleagues who contributed to the individual case studies that we have drawn on. This work received no direct funding, but it has been informed by projects funded by Asthma UK, the NHS Service Delivery Organisation, NHS Connecting for Health Evaluation Programme, and Patient Safety Research Portfolio. We would also like to thank the expert reviewers for their insightful and constructive feedback. Our thanks are also due to Dr. Allison Worth who commented on an earlier draft of this manuscript.
Author information
Authors and affiliations.
Division of Primary Care, The University of Nottingham, Nottingham, UK
Sarah Crowe & Anthony Avery
Centre for Population Health Sciences, The University of Edinburgh, Edinburgh, UK
Kathrin Cresswell, Ann Robertson & Aziz Sheikh
School of Health in Social Science, The University of Edinburgh, Edinburgh, UK
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Sarah Crowe .
Additional information
Competing interests.
The authors declare that they have no competing interests.
Authors' contributions
AS conceived this article. SC, KC and AR wrote this paper with GH, AA and AS all commenting on various drafts. SC and AS are guarantors.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License ( http://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Reprints and permissions
About this article
Cite this article.
Crowe, S., Cresswell, K., Robertson, A. et al. The case study approach. BMC Med Res Methodol 11 , 100 (2011). https://doi.org/10.1186/1471-2288-11-100
Download citation
Received : 29 November 2010
Accepted : 27 June 2011
Published : 27 June 2011
DOI : https://doi.org/10.1186/1471-2288-11-100
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Case Study Approach
- Electronic Health Record System
- Case Study Design
- Case Study Site
- Case Study Report
BMC Medical Research Methodology
ISSN: 1471-2288
- General enquiries: [email protected]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
The PMC website is updating on October 15, 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Int J Prev Med
Qualitative Methods in Health Care Research
Vishnu renjith.
School of Nursing and Midwifery, Royal College of Surgeons Ireland - Bahrain (RCSI Bahrain), Al Sayh Muharraq Governorate, Bahrain
Renjulal Yesodharan
1 Department of Mental Health Nursing, Manipal College of Nursing Manipal, Manipal Academy of Higher Education, Manipal, Karnataka, India
Judith A. Noronha
2 Department of OBG Nursing, Manipal College of Nursing Manipal, Manipal Academy of Higher Education, Manipal, Karnataka, India
Elissa Ladd
3 School of Nursing, MGH Institute of Health Professions, Boston, USA
Anice George
4 Department of Child Health Nursing, Manipal College of Nursing Manipal, Manipal Academy of Higher Education, Manipal, Karnataka, India
Healthcare research is a systematic inquiry intended to generate robust evidence about important issues in the fields of medicine and healthcare. Qualitative research has ample possibilities within the arena of healthcare research. This article aims to inform healthcare professionals regarding qualitative research, its significance, and applicability in the field of healthcare. A wide variety of phenomena that cannot be explained using the quantitative approach can be explored and conveyed using a qualitative method. The major types of qualitative research designs are narrative research, phenomenological research, grounded theory research, ethnographic research, historical research, and case study research. The greatest strength of the qualitative research approach lies in the richness and depth of the healthcare exploration and description it makes. In health research, these methods are considered as the most humanistic and person-centered way of discovering and uncovering thoughts and actions of human beings.
Introduction
Healthcare research is a systematic inquiry intended to generate trustworthy evidence about issues in the field of medicine and healthcare. The three principal approaches to health research are the quantitative, the qualitative, and the mixed methods approach. The quantitative research method uses data, which are measures of values and counts and are often described using statistical methods which in turn aids the researcher to draw inferences. Qualitative research incorporates the recording, interpreting, and analyzing of non-numeric data with an attempt to uncover the deeper meanings of human experiences and behaviors. Mixed methods research, the third methodological approach, involves collection and analysis of both qualitative and quantitative information with an objective to solve different but related questions, or at times the same questions.[ 1 , 2 ]
In healthcare, qualitative research is widely used to understand patterns of health behaviors, describe lived experiences, develop behavioral theories, explore healthcare needs, and design interventions.[ 1 , 2 , 3 ] Because of its ample applications in healthcare, there has been a tremendous increase in the number of health research studies undertaken using qualitative methodology.[ 4 , 5 ] This article discusses qualitative research methods, their significance, and applicability in the arena of healthcare.
Qualitative Research
Diverse academic and non-academic disciplines utilize qualitative research as a method of inquiry to understand human behavior and experiences.[ 6 , 7 ] According to Munhall, “Qualitative research involves broadly stated questions about human experiences and realities, studied through sustained contact with the individual in their natural environments and producing rich, descriptive data that will help us to understand those individual's experiences.”[ 8 ]
Significance of Qualitative Research
The qualitative method of inquiry examines the 'how' and 'why' of decision making, rather than the 'when,' 'what,' and 'where.'[ 7 ] Unlike quantitative methods, the objective of qualitative inquiry is to explore, narrate, and explain the phenomena and make sense of the complex reality. Health interventions, explanatory health models, and medical-social theories could be developed as an outcome of qualitative research.[ 9 ] Understanding the richness and complexity of human behavior is the crux of qualitative research.
Differences between Quantitative and Qualitative Research
The quantitative and qualitative forms of inquiry vary based on their underlying objectives. They are in no way opposed to each other; instead, these two methods are like two sides of a coin. The critical differences between quantitative and qualitative research are summarized in Table 1 .[ 1 , 10 , 11 ]
Differences between quantitative and qualitative research
| Areas | Quantitative Research | Qualitative Research |
|---|---|---|
| Nature of reality | Assumes there is a single reality. | Assumes existence of dynamic and multiple reality. |
| Goal | Test and confirm hypotheses. | Explore and understand phenomena. |
| Data collection methods | Highly structured methods like questionnaires, inventories and scales. | Semi structured like in-depth interviews, observations and focus group discussions. |
| Design | Predetermined and rigid design. | Flexible and emergent design. |
| Reasoning | Deductive process to test the hypothesis. | Primarily inductive to develop the theory or hypothesis. |
| Focus | Concerned with the outcomes and prediction of the causal relationships. | Concerned primarily with process, rather than outcomes or products. |
| Sampling | Rely largely on random sampling methods. | Based on purposive sampling methods. |
| Sample size determination | Involves a-priori sample size calculation. | Collect data until data saturation is achieved. |
| Sample size | Relatively large. | Small sample size but studied in-depth. |
| Data analysis | Variable based and use of statistical or mathematical methods. | Case based and use non statistical descriptive or interpretive methods. |
Qualitative Research Questions and Purpose Statements
Qualitative questions are exploratory and are open-ended. A well-formulated study question forms the basis for developing a protocol, guides the selection of design, and data collection methods. Qualitative research questions generally involve two parts, a central question and related subquestions. The central question is directed towards the primary phenomenon under study, whereas the subquestions explore the subareas of focus. It is advised not to have more than five to seven subquestions. A commonly used framework for designing a qualitative research question is the 'PCO framework' wherein, P stands for the population under study, C stands for the context of exploration, and O stands for the outcome/s of interest.[ 12 ] The PCO framework guides researchers in crafting a focused study question.
Example: In the question, “What are the experiences of mothers on parenting children with Thalassemia?”, the population is “mothers of children with Thalassemia,” the context is “parenting children with Thalassemia,” and the outcome of interest is “experiences.”
The purpose statement specifies the broad focus of the study, identifies the approach, and provides direction for the overall goal of the study. The major components of a purpose statement include the central phenomenon under investigation, the study design and the population of interest. Qualitative research does not require a-priori hypothesis.[ 13 , 14 , 15 ]
Example: Borimnejad et al . undertook a qualitative research on the lived experiences of women suffering from vitiligo. The purpose of this study was, “to explore lived experiences of women suffering from vitiligo using a hermeneutic phenomenological approach.” [ 16 ]
Review of the Literature
In quantitative research, the researchers do an extensive review of scientific literature prior to the commencement of the study. However, in qualitative research, only a minimal literature search is conducted at the beginning of the study. This is to ensure that the researcher is not influenced by the existing understanding of the phenomenon under the study. The minimal literature review will help the researchers to avoid the conceptual pollution of the phenomenon being studied. Nonetheless, an extensive review of the literature is conducted after data collection and analysis.[ 15 ]
Reflexivity
Reflexivity refers to critical self-appraisal about one's own biases, values, preferences, and preconceptions about the phenomenon under investigation. Maintaining a reflexive diary/journal is a widely recognized way to foster reflexivity. According to Creswell, “Reflexivity increases the credibility of the study by enhancing more neutral interpretations.”[ 7 ]
Types of Qualitative Research Designs
The qualitative research approach encompasses a wide array of research designs. The words such as types, traditions, designs, strategies of inquiry, varieties, and methods are used interchangeably. The major types of qualitative research designs are narrative research, phenomenological research, grounded theory research, ethnographic research, historical research, and case study research.[ 1 , 7 , 10 ]
Narrative research
Narrative research focuses on exploring the life of an individual and is ideally suited to tell the stories of individual experiences.[ 17 ] The purpose of narrative research is to utilize 'story telling' as a method in communicating an individual's experience to a larger audience.[ 18 ] The roots of narrative inquiry extend to humanities including anthropology, literature, psychology, education, history, and sociology. Narrative research encompasses the study of individual experiences and learning the significance of those experiences. The data collection procedures include mainly interviews, field notes, letters, photographs, diaries, and documents collected from one or more individuals. Data analysis involves the analysis of the stories or experiences through “re-storying of stories” and developing themes usually in chronological order of events. Rolls and Payne argued that narrative research is a valuable approach in health care research, to gain deeper insight into patient's experiences.[ 19 ]
Example: Karlsson et al . undertook a narrative inquiry to “explore how people with Alzheimer's disease present their life story.” Data were collected from nine participants. They were asked to describe about their life experiences from childhood to adulthood, then to current life and their views about the future life. [ 20 ]
Phenomenological research
Phenomenology is a philosophical tradition developed by German philosopher Edmond Husserl. His student Martin Heidegger did further developments in this methodology. It defines the 'essence' of individual's experiences regarding a certain phenomenon.[ 1 ] The methodology has its origin from philosophy, psychology, and education. The purpose of qualitative research is to understand the people's everyday life experiences and reduce it into the central meaning or the 'essence of the experience'.[ 21 , 22 ] The unit of analysis of phenomenology is the individuals who have had similar experiences of the phenomenon. Interviews with individuals are mainly considered for the data collection, though, documents and observations are also useful. Data analysis includes identification of significant meaning elements, textural description (what was experienced), structural description (how was it experienced), and description of 'essence' of experience.[ 1 , 7 , 21 ] The phenomenological approach is further divided into descriptive and interpretive phenomenology. Descriptive phenomenology focuses on the understanding of the essence of experiences and is best suited in situations that need to describe the lived phenomenon. Hermeneutic phenomenology or Interpretive phenomenology moves beyond the description to uncover the meanings that are not explicitly evident. The researcher tries to interpret the phenomenon, based on their judgment rather than just describing it.[ 7 , 21 , 22 , 23 , 24 ]
Example: A phenomenological study conducted by Cornelio et al . aimed at describing the lived experiences of mothers in parenting children with leukemia. Data from ten mothers were collected using in-depth semi-structured interviews and were analyzed using Husserl's method of phenomenology. Themes such as “pivotal moment in life”, “the experience of being with a seriously ill child”, “having to keep distance with the relatives”, “overcoming the financial and social commitments”, “responding to challenges”, “experience of faith as being key to survival”, “health concerns of the present and future”, and “optimism” were derived. The researchers reported the essence of the study as “chronic illness such as leukemia in children results in a negative impact on the child and on the mother.” [ 25 ]
Grounded Theory Research
Grounded theory has its base in sociology and propagated by two sociologists, Barney Glaser, and Anselm Strauss.[ 26 ] The primary purpose of grounded theory is to discover or generate theory in the context of the social process being studied. The major difference between grounded theory and other approaches lies in its emphasis on theory generation and development. The name grounded theory comes from its ability to induce a theory grounded in the reality of study participants.[ 7 , 27 ] Data collection in grounded theory research involves recording interviews from many individuals until data saturation. Constant comparative analysis, theoretical sampling, theoretical coding, and theoretical saturation are unique features of grounded theory research.[ 26 , 27 , 28 ] Data analysis includes analyzing data through 'open coding,' 'axial coding,' and 'selective coding.'[ 1 , 7 ] Open coding is the first level of abstraction, and it refers to the creation of a broad initial range of categories, axial coding is the procedure of understanding connections between the open codes, whereas selective coding relates to the process of connecting the axial codes to formulate a theory.[ 1 , 7 ] Results of the grounded theory analysis are supplemented with a visual representation of major constructs usually in the form of flow charts or framework diagrams. Quotations from the participants are used in a supportive capacity to substantiate the findings. Strauss and Corbin highlights that “the value of the grounded theory lies not only in its ability to generate a theory but also to ground that theory in the data.”[ 27 ]
Example: Williams et al . conducted a grounded theory research to explore the nature of relationship between the sense of self and the eating disorders. Data were collected form 11 women with a lifetime history of Anorexia Nervosa and were analyzed using the grounded theory methodology. Analysis led to the development of a theoretical framework on the nature of the relationship between the self and Anorexia Nervosa. [ 29 ]
Ethnographic research
Ethnography has its base in anthropology, where the anthropologists used it for understanding the culture-specific knowledge and behaviors. In health sciences research, ethnography focuses on narrating and interpreting the health behaviors of a culture-sharing group. 'Culture-sharing group' in an ethnography represents any 'group of people who share common meanings, customs or experiences.' In health research, it could be a group of physicians working in rural care, a group of medical students, or it could be a group of patients who receive home-based rehabilitation. To understand the cultural patterns, researchers primarily observe the individuals or group of individuals for a prolonged period of time.[ 1 , 7 , 30 ] The scope of ethnography can be broad or narrow depending on the aim. The study of more general cultural groups is termed as macro-ethnography, whereas micro-ethnography focuses on more narrowly defined cultures. Ethnography is usually conducted in a single setting. Ethnographers collect data using a variety of methods such as observation, interviews, audio-video records, and document reviews. A written report includes a detailed description of the culture sharing group with emic and etic perspectives. When the researcher reports the views of the participants it is called emic perspectives and when the researcher reports his or her views about the culture, the term is called etic.[ 7 ]
Example: The aim of the ethnographic study by LeBaron et al . was to explore the barriers to opioid availability and cancer pain management in India. The researchers collected data from fifty-nine participants using in-depth semi-structured interviews, participant observation, and document review. The researchers identified significant barriers by open coding and thematic analysis of the formal interview. [ 31 ]
Historical research
Historical research is the “systematic collection, critical evaluation, and interpretation of historical evidence”.[ 1 ] The purpose of historical research is to gain insights from the past and involves interpreting past events in the light of the present. The data for historical research are usually collected from primary and secondary sources. The primary source mainly includes diaries, first hand information, and writings. The secondary sources are textbooks, newspapers, second or third-hand accounts of historical events and medical/legal documents. The data gathered from these various sources are synthesized and reported as biographical narratives or developmental perspectives in chronological order. The ideas are interpreted in terms of the historical context and significance. The written report describes 'what happened', 'how it happened', 'why it happened', and its significance and implications to current clinical practice.[ 1 , 10 ]
Example: Lubold (2019) analyzed the breastfeeding trends in three countries (Sweden, Ireland, and the United States) using a historical qualitative method. Through analysis of historical data, the researcher found that strong family policies, adherence to international recommendations and adoption of baby-friendly hospital initiative could greatly enhance the breastfeeding rates. [ 32 ]
Case study research
Case study research focuses on the description and in-depth analysis of the case(s) or issues illustrated by the case(s). The design has its origin from psychology, law, and medicine. Case studies are best suited for the understanding of case(s), thus reducing the unit of analysis into studying an event, a program, an activity or an illness. Observations, one to one interviews, artifacts, and documents are used for collecting the data, and the analysis is done through the description of the case. From this, themes and cross-case themes are derived. A written case study report includes a detailed description of one or more cases.[ 7 , 10 ]
Example: Perceptions of poststroke sexuality in a woman of childbearing age was explored using a qualitative case study approach by Beal and Millenbrunch. Semi structured interview was conducted with a 36- year mother of two children with a history of Acute ischemic stroke. The data were analyzed using an inductive approach. The authors concluded that “stroke during childbearing years may affect a woman's perception of herself as a sexual being and her ability to carry out gender roles”. [ 33 ]
Sampling in Qualitative Research
Qualitative researchers widely use non-probability sampling techniques such as purposive sampling, convenience sampling, quota sampling, snowball sampling, homogeneous sampling, maximum variation sampling, extreme (deviant) case sampling, typical case sampling, and intensity sampling. The selection of a sampling technique depends on the nature and needs of the study.[ 34 , 35 , 36 , 37 , 38 , 39 , 40 ] The four widely used sampling techniques are convenience sampling, purposive sampling, snowball sampling, and intensity sampling.
Convenience sampling
It is otherwise called accidental sampling, where the researchers collect data from the subjects who are selected based on accessibility, geographical proximity, ease, speed, and or low cost.[ 34 ] Convenience sampling offers a significant benefit of convenience but often accompanies the issues of sample representation.
Purposive sampling
Purposive or purposeful sampling is a widely used sampling technique.[ 35 ] It involves identifying a population based on already established sampling criteria and then selecting subjects who fulfill that criteria to increase the credibility. However, choosing information-rich cases is the key to determine the power and logic of purposive sampling in a qualitative study.[ 1 ]
Snowball sampling
The method is also known as 'chain referral sampling' or 'network sampling.' The sampling starts by having a few initial participants, and the researcher relies on these early participants to identify additional study participants. It is best adopted when the researcher wishes to study the stigmatized group, or in cases, where findings of participants are likely to be difficult by ordinary means. Respondent ridden sampling is an improvised version of snowball sampling used to find out the participant from a hard-to-find or hard-to-study population.[ 37 , 38 ]
Intensity sampling
The process of identifying information-rich cases that manifest the phenomenon of interest is referred to as intensity sampling. It requires prior information, and considerable judgment about the phenomenon of interest and the researcher should do some preliminary investigations to determine the nature of the variation. Intensity sampling will be done once the researcher identifies the variation across the cases (extreme, average and intense) and picks the intense cases from them.[ 40 ]
Deciding the Sample Size
A-priori sample size calculation is not undertaken in the case of qualitative research. Researchers collect the data from as many participants as possible until they reach the point of data saturation. Data saturation or the point of redundancy is the stage where the researcher no longer sees or hears any new information. Data saturation gives the idea that the researcher has captured all possible information about the phenomenon of interest. Since no further information is being uncovered as redundancy is achieved, at this point the data collection can be stopped. The objective here is to get an overall picture of the chronicle of the phenomenon under the study rather than generalization.[ 1 , 7 , 41 ]
Data Collection in Qualitative Research
The various strategies used for data collection in qualitative research includes in-depth interviews (individual or group), focus group discussions (FGDs), participant observation, narrative life history, document analysis, audio materials, videos or video footage, text analysis, and simple observation. Among all these, the three popular methods are the FGDs, one to one in-depth interviews and the participant observation.
FGDs are useful in eliciting data from a group of individuals. They are normally built around a specific topic and are considered as the best approach to gather data on an entire range of responses to a topic.[ 42 Group size in an FGD ranges from 6 to 12. Depending upon the nature of participants, FGDs could be homogeneous or heterogeneous.[ 1 , 14 ] One to one in-depth interviews are best suited to obtain individuals' life histories, lived experiences, perceptions, and views, particularly while exporting topics of sensitive nature. In-depth interviews can be structured, unstructured, or semi-structured. However, semi-structured interviews are widely used in qualitative research. Participant observations are suitable for gathering data regarding naturally occurring behaviors.[ 1 ]
Data Analysis in Qualitative Research
Various strategies are employed by researchers to analyze data in qualitative research. Data analytic strategies differ according to the type of inquiry. A general content analysis approach is described herewith. Data analysis begins by transcription of the interview data. The researcher carefully reads data and gets a sense of the whole. Once the researcher is familiarized with the data, the researcher strives to identify small meaning units called the 'codes.' The codes are then grouped based on their shared concepts to form the primary categories. Based on the relationship between the primary categories, they are then clustered into secondary categories. The next step involves the identification of themes and interpretation to make meaning out of data. In the results section of the manuscript, the researcher describes the key findings/themes that emerged. The themes can be supported by participants' quotes. The analytical framework used should be explained in sufficient detail, and the analytic framework must be well referenced. The study findings are usually represented in a schematic form for better conceptualization.[ 1 , 7 ] Even though the overall analytical process remains the same across different qualitative designs, each design such as phenomenology, ethnography, and grounded theory has design specific analytical procedures, the details of which are out of the scope of this article.
Computer-Assisted Qualitative Data Analysis Software (CAQDAS)
Until recently, qualitative analysis was done either manually or with the help of a spreadsheet application. Currently, there are various software programs available which aid researchers to manage qualitative data. CAQDAS is basically data management tools and cannot analyze the qualitative data as it lacks the ability to think, reflect, and conceptualize. Nonetheless, CAQDAS helps researchers to manage, shape, and make sense of unstructured information. Open Code, MAXQDA, NVivo, Atlas.ti, and Hyper Research are some of the widely used qualitative data analysis software.[ 14 , 43 ]
Reporting Guidelines
Consolidated Criteria for Reporting Qualitative Research (COREQ) is the widely used reporting guideline for qualitative research. This 32-item checklist assists researchers in reporting all the major aspects related to the study. The three major domains of COREQ are the 'research team and reflexivity', 'study design', and 'analysis and findings'.[ 44 , 45 ]
Critical Appraisal of Qualitative Research
Various scales are available to critical appraisal of qualitative research. The widely used one is the Critical Appraisal Skills Program (CASP) Qualitative Checklist developed by CASP network, UK. This 10-item checklist evaluates the quality of the study under areas such as aims, methodology, research design, ethical considerations, data collection, data analysis, and findings.[ 46 ]
Ethical Issues in Qualitative Research
A qualitative study must be undertaken by grounding it in the principles of bioethics such as beneficence, non-maleficence, autonomy, and justice. Protecting the participants is of utmost importance, and the greatest care has to be taken while collecting data from a vulnerable research population. The researcher must respect individuals, families, and communities and must make sure that the participants are not identifiable by their quotations that the researchers include when publishing the data. Consent for audio/video recordings must be obtained. Approval to be in FGDs must be obtained from the participants. Researchers must ensure the confidentiality and anonymity of the transcripts/audio-video records/photographs/other data collected as a part of the study. The researchers must confirm their role as advocates and proceed in the best interest of all participants.[ 42 , 47 , 48 ]
Rigor in Qualitative Research
The demonstration of rigor or quality in the conduct of the study is essential for every research method. However, the criteria used to evaluate the rigor of quantitative studies are not be appropriate for qualitative methods. Lincoln and Guba (1985) first outlined the criteria for evaluating the qualitative research often referred to as “standards of trustworthiness of qualitative research”.[ 49 ] The four components of the criteria are credibility, transferability, dependability, and confirmability.
Credibility refers to confidence in the 'truth value' of the data and its interpretation. It is used to establish that the findings are true, credible and believable. Credibility is similar to the internal validity in quantitative research.[ 1 , 50 , 51 ] The second criterion to establish the trustworthiness of the qualitative research is transferability, Transferability refers to the degree to which the qualitative results are applicability to other settings, population or contexts. This is analogous to the external validity in quantitative research.[ 1 , 50 , 51 ] Lincoln and Guba recommend authors provide enough details so that the users will be able to evaluate the applicability of data in other contexts.[ 49 ] The criterion of dependability refers to the assumption of repeatability or replicability of the study findings and is similar to that of reliability in quantitative research. The dependability question is 'Whether the study findings be repeated of the study is replicated with the same (similar) cohort of participants, data coders, and context?'[ 1 , 50 , 51 ] Confirmability, the fourth criteria is analogous to the objectivity of the study and refers the degree to which the study findings could be confirmed or corroborated by others. To ensure confirmability the data should directly reflect the participants' experiences and not the bias, motivations, or imaginations of the inquirer.[ 1 , 50 , 51 ] Qualitative researchers should ensure that the study is conducted with enough rigor and should report the measures undertaken to enhance the trustworthiness of the study.
Conclusions
Qualitative research studies are being widely acknowledged and recognized in health care practice. This overview illustrates various qualitative methods and shows how these methods can be used to generate evidence that informs clinical practice. Qualitative research helps to understand the patterns of health behaviors, describe illness experiences, design health interventions, and develop healthcare theories. The ultimate strength of the qualitative research approach lies in the richness of the data and the descriptions and depth of exploration it makes. Hence, qualitative methods are considered as the most humanistic and person-centered way of discovering and uncovering thoughts and actions of human beings.
Financial support and sponsorship
Conflicts of interest.
There are no conflicts of interest.
Our systems are now restored following recent technical disruption, and we’re working hard to catch up on publishing. We apologise for the inconvenience caused. Find out more: https://www.cambridge.org/universitypress/about-us/news-and-blogs/cambridge-university-press-publishing-update-following-technical-disruption
We use cookies to distinguish you from other users and to provide you with a better experience on our websites. Close this message to accept cookies or find out how to manage your cookie settings .
Login Alert
- > Cambridge Handbook of Qualitative Digital Research
- > Case Study Research Revisited

Book contents
- Cambridge Handbook of Qualitative Digital Research
- Copyright page
- Contributors
- Part I Philosophical, Epistemological and Theoretical Considerations
- Part II Methodological Considerations
- Chapter 7 Human Values in a Digital-First World: The Implications for Qualitative Research
- Chapter 8 One Picture to Study One Thousand Words
- Chapter 9 Demystifying the Digital
- Chapter 10 Case Study Research Revisited
- Chapter 11 Social Media Qualitative Research Vignettes
- Chapter 12 Co-Inquiring in a Digital Age
- Part III Illustrative Examples and Emergent Issues
Chapter 10 - Case Study Research Revisited
from Part II - Methodological Considerations
Published online by Cambridge University Press: 08 June 2023
The chapter re-examines the case study research method and its role and contribution to the IS discipline and focuses on the current status of the case study research and the increased digitalization. The advantages of qualitative interpretive cases studies are identified, recent case studies are described and analyzed, and their contributions highlighted. These examples continue to enhance the discipline and sustain the traditional benefits of the case study research through rich data, analysis and understanding the links between people, organizations and technologies, the advancement and expansion of theory, the identification of hidden aspects, and the emergence of new concepts and theorization. Two of the cases use trace data, a type of data emerging as a product of digitalization. While these cases provide contributions, they also challenge the traditional understanding of what a case study is, and the benefits that accrue. The chapter emphasizes the need for mixed-method and multi-method case studies research in addition to trace data to enhance the benefits of the case study research.
Access options
Save book to kindle.
To save this book to your Kindle, first ensure [email protected] is added to your Approved Personal Document E-mail List under your Personal Document Settings on the Manage Your Content and Devices page of your Amazon account. Then enter the ‘name’ part of your Kindle email address below. Find out more about saving to your Kindle .
Note you can select to save to either the @free.kindle.com or @kindle.com variations. ‘@free.kindle.com’ emails are free but can only be saved to your device when it is connected to wi-fi. ‘@kindle.com’ emails can be delivered even when you are not connected to wi-fi, but note that service fees apply.
Find out more about the Kindle Personal Document Service .
- Case Study Research Revisited
- By Boyka Simeonova , Guy Fitzgerald
- Edited by Boyka Simeonova , University of Leicester , Robert D. Galliers , Bentley University, Massachusetts and Warwick Business School
- Book: Cambridge Handbook of Qualitative Digital Research
- Online publication: 08 June 2023
- Chapter DOI: https://doi.org/10.1017/9781009106436.013
Save book to Dropbox
To save content items to your account, please confirm that you agree to abide by our usage policies. If this is the first time you use this feature, you will be asked to authorise Cambridge Core to connect with your account. Find out more about saving content to Dropbox .
Save book to Google Drive
To save content items to your account, please confirm that you agree to abide by our usage policies. If this is the first time you use this feature, you will be asked to authorise Cambridge Core to connect with your account. Find out more about saving content to Google Drive .

Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
29 Conceptualization in qualitative research
Chapter outline
- 15.1 Alternative paradigms: Interpretivism, critical paradigm, and pragmatism
15.2 Multiparadigmatic research: An example
15.3 idiographic causal relationships, 15.4 qualitative research questions.
Now let’s change things up! In the previous chapters, we explored steps to create and carry out a quantitative research study. Quantitative studies are great when we want to summarize or test relationships between ideas using numbers and the power of statistics. However, qualitative research offers us a different and equally important tool. Sometimes the aim of research projects is to explore meaning and lived experience. Instead of trying to arrive at generalizable conclusions for all people, some research projects establish a deep, authentic description of a specific time, place, and group of people.
Qualitative research relies on the power of human expression through words, pictures, movies, performance and other artifacts that represent these things. All of these tell stories about the human experience and we want to learn from them and have them be represented in our research. Generally speaking, qualitative research is about the gathering up of these stories, breaking them into pieces so we can examine the ideas that make them up, and putting them back together in a way that allows us to tell a common or shared story that responds to our research question. To do that, we need to discuss the assumptions underlying social science.

17.1 Alternative paradigms: Interpretivism, critical, and pragmatism
Learning objectives.
Students will be able to…
- Distinguish between the assumptions of positivism, interpretivism, critical, and pragmatist research paradigms.
- Use paradigm to describe how scientific thought changes over time.
In Chapter 10, we reviewed the assumptions that underly post-positivism (abbreviated hereafter as positivism for brevity). Quantitative methods are most often the choice for positivist research questions because they conform to these assumptions. Qualitative methods can conform to these assumptions; however, they are limited in their generalizability.
Kivunja & Kuyini (2017) [1] describe the essential features of positivism as:
- A belief that theory is universal and law-like generalizations can be made across contexts
- The assumption that context is not important
- The belief that truth or knowledge is ‘out there to be discovered’ by research
- The belief that cause and effect are distinguishable and analytically separable
- The belief that results of inquiry can be quantified
- The belief that theory can be used to predict and to control outcomes
- The belief that research should follow the scientific method of investigation
- Rests on formulation and testing of hypotheses
- Employs empirical or analytical approaches
- Pursues an objective search for facts
- Believes in ability to observe knowledge
- The researcher’s ultimate aim is to establish a comprehensive universal theory, to account for human and social behavior
- Application of the scientific method
Because positivism is the dominant social science research paradigm, it can be easy to ignore or be confused by research that does not use these assumptions. We covered in Chapter 10 the table reprinted below when discussing the assumptions underlying positivistic social science.
As you consider your research project, keep these philosophical assumptions in mind. They are useful shortcuts to understanding the deeper ideas and assumptions behind the construction of knowledge. The purpose of exploring these philosophical assumptions isn’t to find out which is true and which is false. Instead, the goal is to identify the assumptions that fit with how you think about your research question. Choosing a paradigm helps you make those assumptions explicit.
| Ontology: assumptions about what is real | |
| Epistemology: assumptions about how we come to know what is real |
|
| Assumptions about the researcher |
|
| Assumptions about human action |
|
| Assumptions about the social world | |
| Assumptions about the purpose of research |
|
Before we explore alternative paradigms, it’s important for us to review what paradigms are.
How do scientific ideas change over time?
Much like your ideas develop over time as you learn more, so does the body of scientific knowledge. Kuhn’s (1962) [2] The Structure of Scientific Revolutions is one of the most influential works on the philosophy of science, and is credited with introducing the idea of competing paradigms (or “disciplinary matrices”) in research. Kuhn investigated the way that scientific practices evolve over time, arguing that we don’t have a simple progression from “less knowledge” to “more knowledge” because the way that we approach inquiry is changing over time. This can happen gradually, but the process results in moments of change where our understanding of a phenomenon changes more radically (such as in the transition from Newtonian to Einsteinian physics; or from Lamarckian to Darwinian theories of evolution). For a social work practice example, Fleuridas & Krafcik (2019) [3] trace the development of the “four forces” of psychotherapy , from psychodynamics to behaviorism to humanism as well as the competition among emerging perspectives to establish itself as the fourth force to guide psychotherapeutic practice. But how did the problems in one paradigm inspire new paradigms? Kuhn presents us with a way of understanding the history of scientific development across all topics and disciplines.
As you can see in this video from Matthew J. Brown (CC-BY), there are four stages in the cycle of science in Kuhn’s approach. Firstly, a pre-paradigmatic state where competing approaches share no consensus. Secondly, the “normal” state where there is wide acceptance of a particular set of methods and assumptions. Thirdly, a state of crisis where anomalies that cannot be solved within the existing paradigm emerge and competing theories to address them follow. Fourthly, a revolutionary phase where some new paradigmatic approach becomes dominant and supplants the old. Shnieder (2009) [4] suggests that the Kuhnian phases are characterized by different kinds of scientific activity.
Newer approaches often build upon rather than replace older ones, but they also overlap and can exist within a state of competition. Scientists working within a particular paradigm often share methods, assumptions and values. In addition to supporting specific methods, research paradigms also influence things like the ambition and nature of research, the researcher-participant relationship and how the role of the researcher is understood.
Paradigm vs. theory
The terms ‘ paradigm ‘ and ‘ theory ‘ are often used interchangeably in social science. There is not a consensus among social scientists as to whether these are identical or distinct concepts. With that said, in this text, we will make a clear distinction between the two ideas because thinking about each concept separately is more useful for our purposes.
We define paradigm a set of common philosophical (ontological, epistemological, and axiological) assumptions that inform research. The four paradigms we describe in this section refer to patterns in how groups of researchers resolve philosophical questions. Some assumptions naturally make sense together, and paradigms grow out of researchers with shared assumptions about what is important and how to study it. Paradigms are like “analytic lenses” and a provide framework on top of which we can build theoretical and empirical knowledge (Kuhn, 1962). [5] Consider this video of an interview with world-famous physicist Richard Feynman in which he explains why “when you explain a ‘why,’ you have to be in some framework that you allow something to be true. Otherwise, you are perpetually asking why.” In order to answer basic physics question like “what is happening when two magnets attract?” or a social work research question like “what is the impact of this therapeutic intervention on depression,” you must understand the assumptions you are making about social science and the social world. Paradigmatic assumptions about objective and subjective truth support methodological choices like whether to conduct interviews or send out surveys, for example.
While paradigms are broad philosophical assumptions, theory is more specific, and refers to a set of concepts and relationships scientists use to explain the social world. Theories are more concrete, while paradigms are more abstract. Look back to Figure 7.1 at the beginning of this chapter. Theory helps you identify the concepts and relationships that align with your paradigmatic understanding of the problem. Moreover, theory informs how you will measure the concepts in your research question and the design of your project.
For both theories and paradigms, Kuhn’s observation of scientific paradigms, crises, and revolutions is instructive for understanding the history of science. Researchers inherit institutions, norms, and ideas that are marked by the battlegrounds of theoretical and paradigmatic debates that stretch back hundreds of years. We have necessarily simplified this history into four paradigms: positivism, interpretivism, critical, and pragmatism. Our framework and explanation are inspired by the framework of Guba and Lincoln (1990) [6] and Burrell and Morgan (1979). [7] while also incorporating pragmatism as a way of resolving paradigmatic questions. Most of social work research and theory can be classified as belonging to one of these four paradigms, though this classification system represents only one of many useful approaches to analyzing social science research paradigms.
Building on our discussion in section 7.1 on objective vs. subjective epistemologies and ontologies, we will start with the difference between positivism and interpretivism. Afterward, we will link our discussion of axiology in section 7.2 with the critical paradigm. Finally, we will situate pragmatism as a way to resolve paradigmatic questions strategically. The difference between positivism and interpretivism is a good place to start, since the critical paradigm and pragmatism build on their philosophical insights.
It’s important to think of paradigms less as distinct categories and more as a spectrum along which projects might fall. For example, some projects may be somewhat positivist, somewhat interpretivist, and a little critical. No project fits perfectly into one paradigm. Additionally, there is no paradigm that is more correct than the other. Each paradigm uses assumptions that are logically consistent, and when combined, are a useful approach to understanding the social world using science. The purpose of this section is to acquaint you with what research projects in each paradigm look like and how they are grounded in philosophical assumptions about social science.
You should read this section to situate yourself in terms of what paradigm feels most “at home” to both you as a person and to your project. You may find, as I have, that your research projects are more conventional and less radical than what feels most like home to you, personally. In a research project, however, students should start with their working question rather than their heart. Use the paradigm that fits with your question the best, rather than which paradigm you think fits you the best.

Interpretivism: Researcher as “empathizer”
Positivism is focused on generalizable truth. Interpretivism , by contrast, develops from the idea that we want to understand the truths of individuals, how they interpret and experience the world, their thought processes, and the social structures that emerge from sharing those interpretations through language and behavior. The process of interpretation (or social construction) is guided by the empathy of the researcher to understand the meaning behind what other people say.
Historically, interpretivism grew out of a specific critique of positivism: that knowledge in the human and social sciences cannot conform to the model of natural science because there are features of human experience that cannot objectively be “known”. The tools we use to understand objects that have no self-awareness may not be well-attuned to subjective experiences like emotions, understandings, values, feelings, socio-cultural factors, historical influences, and other meaningful aspects of social life. Instead of finding a single generalizable “truth,” the interpretivist researcher aims to generate understanding and often adopts a relativist position.
While positivists seek “the truth,” the social constructionist framework argues that “truth” varies. Truth differs based on who you ask, and people change what they believe is true based on social interactions. These subjective truths also exist within social and historical contexts, and our understanding of truth varies across communities and time periods. This is because we, according to this paradigm, create reality ourselves through our social interactions and our interpretations of those interactions. Key to the interpretivist perspective is the idea that social context and interaction frame our realities.
Researchers operating within this framework take keen interest in how people come to socially agree, or disagree, about what is real and true. Consider how people, depending on their social and geographical context, ascribe different meanings to certain hand gestures. When a person raises their middle finger, those of us in Western cultures will probably think that this person isn’t very happy (not to mention the person at whom the middle finger is being directed!). In other societies around the world, a thumbs-up gesture, rather than a middle finger, signifies discontent (Wong, 2007). [8] The fact that these hand gestures have different meanings across cultures aptly demonstrates that those meanings are socially and collectively constructed. What, then, is the “truth” of the middle finger or thumbs up? As we’ve seen in this section, the truth depends on the intention of the person making the gesture, the interpretation of the person receiving it, and the social context in which the action occurred.
Qualitative methods are preferred as ways to investigate these phenomena. Data collected might be unstructured (or “messy”) and correspondingly a range of techniques for approaching data collection have been developed. Interpretivism acknowledges that it is impossible to remove cultural and individual influence from research, often instead making a virtue of the positionality of the researcher and the socio-cultural context of a study.
One common objection positivists levy against interpretivists is that interpretivism tends to emphasize the subjective over the objective. If the starting point for an investigation is that we can’t fully and objectively know the world, how can we do research into this without everything being a matter of opinion? For the positivist, this risk for confirmation bias as well as invalid and unreliable measures makes interpretivist research unscientific. Clearly, we disagree with this assessment, and you should, too. Positivism and interpretivism have different ontologies and epistemologies with contrasting notions of rigor and validity (for more information on assumptions about measurement, see Chapter 11 for quantitative validity and reliability and Chapter 20 for qualitative rigor). Nevertheless, both paradigms apply the values and concepts of the scientific method through systematic investigation of the social world, even if their assumptions lead them to do so in different ways. Interpretivist research often embraces a relativist epistemology, bringing together different perspectives in search of a trustworthy and authentic understanding or narrative.
Kivunja & Kuyini (2017) [9] describe the essential features of interpretivism as:
- The belief that truths are multiple and socially constructed
- The acceptance that there is inevitable interaction between the researcher and his or her research participants
- The acceptance that context is vital for knowledge and knowing
- The belief that knowledge can be value laden and the researcher’s values need to be made explicit
- The need to understand specific cases and contexts rather deriving universal laws that apply to everyone, everywhere.
- The belief that causes and effects are mutually interdependent, and that causality may be circular or contradictory
- The belief that contextual factors need to be taken into consideration in any systematic pursuit of understanding
One important clarification: it’s important to think of the interpretivist perspective as not just about individual interpretations but the social life of interpretations. While individuals may construct their own realities, groups—from a small one such as a married couple to large ones such as nations—often agree on notions of what is true and what “is” and what “is not.” In other words, the meanings that we construct have power beyond the individuals who create them. Therefore, the ways that people and communities act based on such meanings is of as much interest to interpretivists as how they were created in the first place. Theories like social constructionism, phenomenology, and symbolic interactionism are often used in concert with interpretivism.
Is interpretivism right for your project?
An interpretivist orientation to research is appropriate when your working question asks about subjective truths. The cause-and-effect relationships that interpretivist studies produce are specific to the time and place in which the study happened, rather than a generalizable objective truth. More pragmatically, if you picture yourself having a conversation with participants like an interview or focus group, then interpretivism is likely going to be a major influence for your study.
Positivists critique the interpretivist paradigm as non-scientific. They view the interpretivist focus on subjectivity and values as sources of bias. Positivists and interpretivists differ on the degree to which social phenomena are like natural phenomena. Positivists believe that the assumptions of the social sciences and natural sciences are the same, while interpretivists strongly believe that social sciences differ from the natural sciences because their subjects are social creatures.
Similarly, the critical paradigm finds fault with the interpretivist focus on the status quo rather than social change. Although interpretivists often proceed from a feminist or other standpoint theory, the focus is less on liberation than on understanding the present from multiple perspectives. Other critical theorists may object to the consensus orientation of interpretivist research. By searching for commonalities between people’s stories, they may erase the uniqueness of each individual’s story. For example, while interpretivists may arrive at a consensus definition of what the experience of “coming out” is like for people who identify as lesbian, gay, bisexual, transgender, or queer, it cannot represent the diversity of each person’s unique “coming out” experience and what it meant to them. For example, see Rosario and colleagues’ (2009) [10] critique the literature on lesbians “coming out” because previous studies did not addressing how appearing, behaving, or identifying as a butch or femme impacted the experience of “coming out” for lesbians.
- From your literature search, identify an empirical article that uses qualitative methods to answer a research question similar to your working question or about your research topic.
- Review the assumptions of the interpretivist research paradigm.
- Discuss in a few sentences how the author’s conclusions are based on some of these paradigmatic assumptions. How might a researcher operating from a different paradigm (like positivism or the critical paradigm) critique the conclusions of this study?

Critical paradigm: Researcher as “activist”
As we’ve discussed a bit in the preceding sections, the critical paradigm focuses on power, inequality, and social change. Although some rather diverse perspectives are included here, the critical paradigm, in general, includes ideas developed by early social theorists, such as Max Horkheimer (Calhoun et al., 2007), [11] and later works developed by feminist scholars, such as Nancy Fraser (1989). [12] Unlike the positivist paradigm, the critical paradigm assumes that social science can never be truly objective or value-free. Furthermore, this paradigm operates from the perspective that scientific investigation should be conducted with the express goal of social change. Researchers in the critical paradigm foreground axiology, positionality and values . In contrast with the detached, “objective” observations associated with the positivist researcher, critical approaches make explicit the intention for research to act as a transformative or emancipatory force within and beyond the study.
Researchers in the critical paradigm might start with the knowledge that systems are biased against certain groups, such as women or ethnic minorities, building upon previous theory and empirical data. Moreover, their research projects are designed not only to collect data, but to impact the participants as well as the systems being studied. The critical paradigm applies its study of power and inequality to change those power imbalances as part of the research process itself. If this sounds familiar to you, you may remember hearing similar ideas when discussing social conflict theory in your human behavior in the social environment (HBSE) class. [13] Because of this focus on social change, the critical paradigm is a natural home for social work research. However, we fall far short of adopting this approach widely in our profession’s research efforts.
Is the critical paradigm right for your project?
Every social work research project impacts social justice in some way. What distinguishes critical research is how it integrates an analysis of power into the research process itself. Critical research is appropriate for projects that are activist in orientation. For example, critical research projects should have working questions that explicitly seek to raise the consciousness of an oppressed group or collaborate equitably with community members and clients to addresses issues of concern. Because of their transformative potential, critical research projects can be incredibly rewarding to complete. However, partnerships take a long time to develop and social change can evolve slowly on an issue, making critical research projects a more challenging fit for student research projects which must be completed under a tight deadline with few resources.
Positivists critique the critical paradigm on multiple fronts. First and foremost, the focus on oppression and values as part of the research process is seen as likely to bias the research process, most problematically, towards confirmation bias. If you start out with the assumption that oppression exists and must be dealt with, then you are likely to find that regardless of whether it is truly there or not. Similarly, positivists may fault critical researchers for focusing on how the world should be, rather than how it truly is . In this, they may focus too much on theoretical and abstract inquiry and less on traditional experimentation and empirical inquiry. Finally, the goal of social transformation is seen as inherently unscientific, as science is not a political practice.
Interpretivists often find common cause with critical researchers. Feminist studies, for example, may explore the perspectives of women while centering gender-based oppression as part of the research process. In interpretivist research, the focus is less on radical change as part of the research process and more on small, incremental changes based on the results and conclusions drawn from the research project. Additionally, some critical researchers’ focus on individuality of experience is in stark contrast to the consensus-orientation of interpretivists. Interpretivists seek to understand people’s true selves. Some critical theorists argue that people have multiple selves or no self at all.
- From your literature search, identify an article relevant to your working question or broad research topic that uses a critical perspective. You should look for articles where the authors are clear that they are applying a critical approach to research like feminism, anti-racism, Marxism and critical theory, decolonization, anti-oppressive practice, or other social justice-focused theoretical perspectives. To target your search further, include keywords in your queries to research methods commonly used in the critical paradigm like participatory action research and community-based participatory research. If you have trouble identifying an article for this exercise, consult your professor for some help. These articles may be more challenging to find, but reviewing one is necessary to get a feel for what research in this paradigm is like.
- Review the assumptions of the critical research paradigm.
- Discuss in a few sentences how the author’s conclusions are based on some of these paradigmatic assumptions. How might a researcher operating from different assumptions (like values-neutrality or researcher as neutral and unbiased) critique the conclusions of this study?

Pragmatism: Researcher as “strategist”
“Essentially, all models are wrong but some are useful.” (Box, 1976) [14]
Pragmatism is a research paradigm that suspends questions of philosophical ‘truth’ and focuses more on how different philosophies, theories, and methods can be used strategically to provide a multidimensional view of a topic. Researchers employing pragmatism will mix elements of positivist, interpretivist, and critical research depending on the purpose of a particular project and the practical constraints faced by the researcher and their research context. We favor this approach for student projects because it avoids getting bogged down in choosing the “right” paradigm and instead focuses on the assumptions that help you answer your question, given the limitations of your research context. Student research projects are completed quickly and moving in the direction of pragmatism can be a route to successfully completing a project. Your project is a representation of what you think is feasible, ethical, and important enough for you to study.
The crucial consideration for the pragmatist is whether the outcomes of research have any real-world application, rather than whether they are “true.” The methods, theories, and philosophies chosen by pragmatic researchers are guided by their working question. There are no distinctively pragmatic research methods since this approach is about making judicious use whichever methods fit best with the problem under investigation. Pragmatic approaches may be less likely to prioritize ontological, epistemological or axiological consistency when combining different research methods. Instead, the emphasis is on solving a pressing problem and adapting to the limitations and opportunities in the researchers’ context.
Adopt a multi-paradigmatic perspective
Believe it or not, there is a long literature of acrimonious conflict between scientists from positivist, interpretivist, and critical camps (see Heineman-Pieper et al., 2002 [15] for a longer discussion). Pragmatism is an old idea, but it is appealing precisely because it attempts to resolve the problem of multiple incompatible philosophical assumptions in social science. To a pragmatist, there is no “correct” paradigm. All paradigms rely on assumptions about the social world that are the subject of philosophical debate. Each paradigm is an incomplete understanding of the world, and it requires a scientific community using all of them to gain a comprehensive view of the social world. This multi-paradigmatic perspective is a unique gift of social work research, as our emphasis on empathy and social change makes us more critical of positivism, the dominant paradigm in social science.
We offered the metaphors of expert, empathizer, activist, and strategist for each paradigm. It’s important not to take these labels too seriously. For example, some may view that scientists should be experts or that activists are biased and unscientific. Nevertheless, we hope that these metaphors give you a sense of what it feels like to conduct research within each paradigm.
One of the unique aspects of paradigmatic thinking is that often where you think you are most at home may actually be the opposite of where your research project is. For example, in my graduate and doctoral education, I thought I was a critical researcher. In fact, I thought I was a radical researcher focused on social change and transformation. Yet, often times when I sit down to conceptualize and start a research project, I find myself squarely in the positivist paradigm, thinking through neat cause-and-effect relationships that can be mathematically measured. There is nothing wrong with that! Your task for your research project is to find the paradigm that best matches your research question. Think through what you really want to study and how you think about the topic, then use assumptions of that paradigm to guide your inquiry.
Another important lesson is that no research project fits perfectly in one paradigm or another. Instead, there is a spectrum along which studies are, to varying degrees, interpretivist, positivist, and critical. For example, all social work research is a bit activist in that our research projects are designed to inform action for change on behalf of clients and systems. However, some projects will focus on the conclusions and implications of projects informing social change (i.e., positivist and interpretivist projects) while others will partner with community members and design research projects collaboratively in a way that leads to social change (i.e. critical projects). In section 7.5, we will describe a pragmatic approach to research design guided by your paradigmatic and theoretical framework.
Key Takeaways
- Social work research falls, to some degree, in each of the four paradigms: positivism, interpretivism, critical, and pragmatist.
- Adopting a pragmatic, multi-paradigmatic approach to research makes sense for student researchers, as it directs students to use the philosophical assumptions and methodological approaches that best match their research question and research context.
- Research in all paradigms is necessary to come to a comprehensive understanding of a topic, and social workers must be able to understand and apply knowledge from each research paradigm.
- Describe which paradigm best fits your perspective on the world and which best fits with your project.
- Identify any similarities and differences in your personal assumptions and the assumption your research project relies upon. For example, are you a more critical and radical thinker but have chosen a more “expert” role for yourself in your research project?
Learners will be able to…
- Apply the assumptions of each paradigm to your project
- Summarize what aspects of your project stem from positivist, interpretivist, or critical assumptions
In the previous sections, we reviewed the major paradigms and theories in social work research. In this section, we will provide an example of how to apply theory and paradigm in research. This process is depicted in Figure 7.2 below with some quick summary questions for each stage. Some questions in the figure below have example answers like designs (i.e., experimental, survey) and data analysis approaches (i.e., discourse analysis). These examples are arbitrary. There are a lot of options that are not listed. So, don’t feel like you have to memorize them or use them in your study.
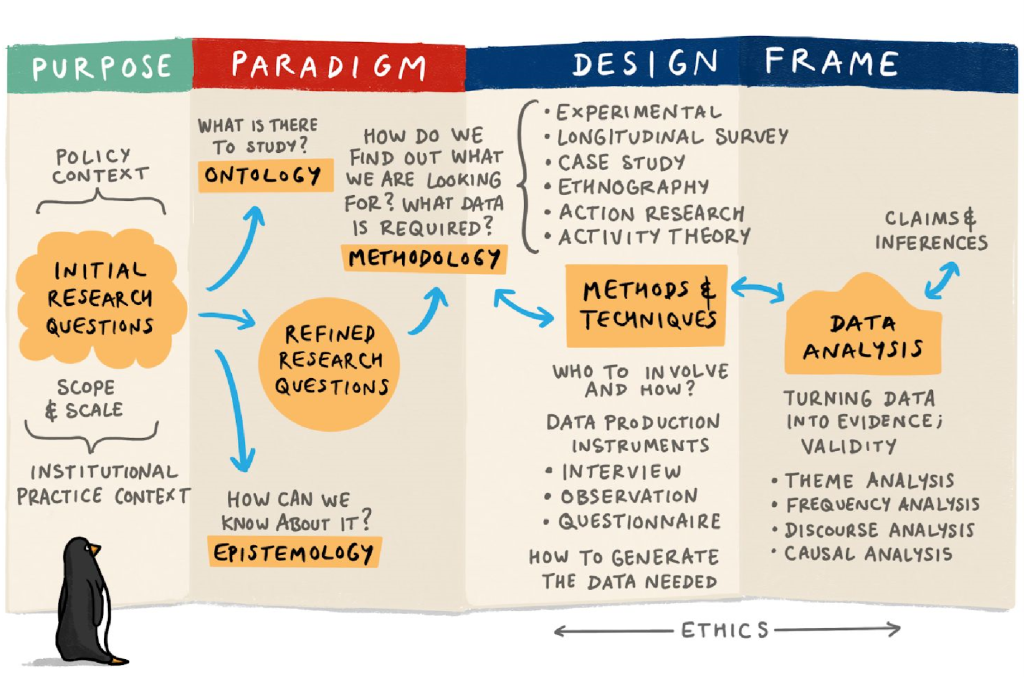
This diagram (taken from an archived Open University (UK) course entitled E89 - Educational Inquiry ) shows one way to visualize the research design process. While research is far from linear, in general, this is how research projects progress sequentially. Researchers begin with a working question, and through engaging with the literature, develop and refine those questions into research questions (a process we will finalize in Chapter 9 ). But in order to get to the part where you gather your sample, measure your participants, and analyze your data, you need to start with paradigm. Based on your work in section 7.3, you should have a sense of which paradigm or paradigms are best suited to answering your question. The approach taken will often reflect the nature of the research question; the kind of data it is possible to collect; and work previously done in the area under consideration. When evaluating paradigm and theory, it is important to look at what other authors have done previously and the framework used by studies that are similar to the one you are thinking of conducting.
Once you situate your project in a research paradigm, it becomes possible to start making concrete choices about methods. Depending on the project, this will involve choices about things like:
- What is my final research question?
- What are the key variables and concepts under investigation, and how will I measure them?
- How do I find a representative sample of people who experience the topic I’m studying?
- What design is most appropriate for my research question?
- How will I collect and analyze data?
- How do I determine whether my results describe real patterns in the world or are the result of bias or error?
The data collection phase can begin once these decisions are made. It can be very tempting to start collecting data as soon as possible in the research process as this gives a sense of progress. However, it is usually worth getting things exactly right before collecting data as an error found in your approach further down the line can be harder to correct or recalibrate around.
Designing a study using paradigm and theory: An example
Paradigm and theory have the potential to turn some people off since there is a lot of abstract terminology and thinking about real-world social work practice contexts. In this section, I’ll use an example from my own research, and I hope it will illustrate a few things. First, it will show that paradigms are really just philosophical statements about things you already understand and think about normally. It will also show that no project neatly sits in one paradigm and that a social work researcher should use whichever paradigm or combination of paradigms suit their question the best. Finally, I hope it is one example of how to be a pragmatist and strategically use the strengths of different theories and paradigms to answering a research question. We will pick up the discussion of mixed methods in the next chapter.
Thinking as an expert: Positivism
In my undergraduate research methods class, I used an open textbook much like this one and wanted to study whether it improved student learning. You can read a copy of the article we wrote on based on our study . We’ll learn more about the specifics of experiments and evaluation research in Chapter 13 , but you know enough to understand what evaluating an intervention might look like. My first thought was to conduct an experiment, which placed me firmly within the positivist or “expert” paradigm.
Experiments focus on isolating the relationship between cause and effect. For my study, this meant studying an open textbook (the cause, or intervention) and final grades (the effect, or outcome). Notice that my position as “expert” lets me assume many things in this process. First, it assumes that I can distill the many dimensions of student learning into one number—the final grade. Second, as the “expert,” I’ve determined what the intervention is: indeed, I created the book I was studying, and applied a theory from experts in the field that explains how and why it should impact student learning.
Theory is part of applying all paradigms, but I’ll discuss its impact within positivism first. Theories grounded in positivism help explain why one thing causes another. More specifically, these theories isolate a causal relationship between two (or more) concepts while holding constant the effects of other variables that might confound the relationship between the key variables. That is why experimental design is so common in positivist research. The researcher isolates the environment from anything that might impact or bias the cause and effect relationship they want to investigate.
But in order for one thing to lead to change in something else, there must be some logical, rational reason why it would do so. In open education, there are a few hypotheses (though no full-fledged theories) on why students might perform better using open textbooks. The most common is the access hypothesis , which states that students who cannot afford expensive textbooks or wouldn’t buy them anyway can access open textbooks because they are free, which will improve their grades. It’s important to note that I held this theory prior to starting the experiment, as in positivist research you spell out your hypotheses in advance and design an experiment to support or refute that hypothesis.
Notice that the hypothesis here applies not only to the people in my experiment, but to any student in higher education. Positivism seeks generalizable truth, or what is true for everyone. The results of my study should provide evidence that anyone who uses an open textbook would achieve similar outcomes. Of course, there were a number of limitations as it was difficult to tightly control the study. I could not randomly assign students or prevent them from sharing resources with one another, for example. So, while this study had many positivist elements, it was far from a perfect positivist study because I was forced to adapt to the pragmatic limitations of my research context (e.g., I cannot randomly assign students to classes) that made it difficult to establish an objective, generalizable truth.
Thinking like an empathizer: Interpretivism
One of the things that did not sit right with me about the study was the reliance on final grades to signify everything that was going on with students. I added another quantitative measure that measured research knowledge, but this was still too simplistic. I wanted to understand how students used the book and what they thought about it. I could create survey questions that ask about these things, but to get at the subjective truths here, I thought it best to use focus groups in which students would talk to one another with a researcher moderating the discussion and guiding it using predetermined questions. You will learn more about focus groups in Chapter 18 .
Researchers spoke with small groups of students during the last class of the semester. They prompted people to talk about aspects of the textbook they liked and didn’t like, compare it to textbooks from other classes, describe how they used it, and so forth. It was this focus on understanding and subjective experience that brought us into the interpretivist paradigm. Alongside other researchers, I created the focus group questions but encouraged researchers who moderated the focus groups to allow the conversation to flow organically.
We originally started out with the assumption, for which there is support in the literature, that students would be angry with the high-cost textbook that we used prior to the free one, and this cost shock might play a role in students’ negative attitudes about research. But unlike the hypotheses in positivism, these are merely a place to start and are open to revision throughout the research process. This is because the researchers are not the experts, the participants are! Just like your clients are the experts on their lives, so were the students in my study. Our job as researchers was to create a group in which they would reveal their informed thoughts about the issue, coming to consensus around a few key themes.

When we initially analyzed the focus groups, we uncovered themes that seemed to fit the data. But the overall picture was murky. How were themes related to each other? And how could we distill these themes and relationships into something meaningful? We went back to the data again. We could do this because there isn’t one truth, as in positivism, but multiple truths and multiple ways of interpreting the data. When we looked again, we focused on some of the effects of having a textbook customized to the course. It was that customization process that helped make the language more approachable, engaging, and relevant to social work practice.
Ultimately, our data revealed differences in how students perceived a free textbook versus a free textbook that is customized to the class. When we went to interpret this finding, the remix hypothesis of open textbook was helpful in understanding that relationship. It states that the more faculty incorporate editing and creating into the course, the better student learning will be. Our study helped flesh out that theory by discussing the customization process and how students made sense of a customized resource.
In this way, theoretical analysis operates differently in interpretivist research. While positivist research tests existing theories, interpretivist research creates theories based on the stories of research participants. However, it is difficult to say if this theory was totally emergent in the dataset or if my prior knowledge of the remix hypothesis influenced my thinking about the data. Interpretivist researchers are encouraged to put a box around their prior experiences and beliefs, acknowledging them, but trying to approach the data with fresh eyes. Interpretivists know that this is never perfectly possible, though, as we are always influenced by our previous experiences when interpreting data and conducting scientific research projects.
Thinking like an activist: Critical
Although adding focus groups helped ease my concern about reducing student learning down to just final grades by providing a more rich set of conversations to analyze. However, my role as researcher and “expert” was still an important part of the analysis. As someone who has been out of school for a while, and indeed has taught this course for years, I have lost touch with what it is like to be a student taking research methods for the first time. How could I accurately interpret or understand what students were saying? Perhaps I would overlook things that reflected poorly on my teaching or my book. I brought other faculty researchers on board to help me analyze the data, but this still didn’t feel like enough.
By luck, an undergraduate student approached me about wanting to work together on a research project. I asked her if she would like to collaborate on evaluating the textbook with me. Over the next year, she assisted me with conceptualizing the project, creating research questions, as well as conducting and analyzing the focus groups. Not only would she provide an “insider” perspective on coding the data, steeped in her lived experience as a student, but she would serve as a check on my power through the process.
Including people from the group you are measuring as part of your research team is a common component of critical research. Ultimately, critical theorists would find my study to be inadequate in many ways. I still developed the research question, created the intervention, and wrote up the results for publication, which privileges my voice and role as “expert.” Instead, critical theorists would emphasize the role of students (community members) in identifying research questions, choosing the best intervention to used, and so forth. But collaborating with students as part of a research team did address some of the power imbalances in the research process.
Critical research projects also aim to have an impact on the people and systems involved in research. No students or researchers had profound personal realizations as a result of my study, nor did it lessen the impact of oppressive structures in society. I can claim some small victory that my department switched to using my textbook after the study was complete (changing a system), though this was likely the result of factors other than the study (my advocacy for open textbooks).
Social work research is almost always designed to create change for people or systems. To that end, every social work project is at least somewhat critical. However, the additional steps of conducting research with people rather than on people reveal a depth to the critical paradigm. By bringing students on board the research team, study had student perspectives represented in conceptualization, data collection, and analysis. That said, there was much to critique about this study from a critical perspective. I retained a lot of the power in the research process, and students did not have the ability to determine the research question or purpose of the project. For example, students might likely have said that textbook costs and the quality of their research methods textbook were less important than student debt, racism, or other potential issues experienced by students in my class. Instead of a ground-up research process based in community engagement, my research included some important participation by students on project created and led by faculty.
Conceptualization is an iterative process
I hope this conversation was useful in applying paradigms to a research project. While my example discusses education research, the same would apply for social work research about social welfare programs, clinical interventions, or other topics. Paradigm and theory are covered at the beginning of the conceptualization of your project because these assumptions will structure the rest of your project. Each of the research steps that occur after this chapter (e.g., forming a question, choosing a design) rely upon philosophical and theoretical assumptions. As you continue conceptualizing your project over the next few weeks, you may find yourself shifting between paradigms. That is normal, as conceptualization is not a linear process. As you move through the next steps of conceptualizing and designing a project, you’ll find philosophies and theories that best match how you want to study your topic.
Viewing theoretical and empirical arguments through this lens is one of the true gifts of the social work approach to research. The multi-paradigmatic perspective is a hallmark of social work research and one that helps us contribute something unique on research teams and in practice.
- Multi-paradigmatic research is a distinguishing hallmark of social work research. Understanding the limitations and strengths of each paradigm will help you justify your research approach and strategically choose elements from one or more paradigms to answer your question.
- Paradigmatic assumptions help you understand the “blind spots” in your research project and how to adjust and address these areas. Keep in mind, it is not necessary to address all of your blind spots, as all projects have limitations.
- Sketch out which paradigm applies best to your project. Second, building on your answer to the exercise in section 7.3, identify how the theory you chose and the paradigm in which you find yourself are consistent or are in conflict with one another. For example, if you are using systems theory in a positivist framework, you might talk about how they both rely on a deterministic approach to human behavior with a focus on the status-quo and social order.
- Define and provide an example of an idiographic causal explanation
- Differentiate between idiographic and nomothetic causal relationships
- Link idiographic and nomothetic causal relationships with the process of theory building and theory testing
- Describe how idiographic and nomothetic causal explanations can be complementary
As we transition away from positivism, it is important to highlight the assumptions it makes about the scientific process–the hypothetico-deductive method, sometimes referred to as the research circle.
The hypothetico-deductive method
The primary way that researchers in the positivist paradigm use theories is sometimes called the hypothetico-deductive method (although this term is much more likely to be used by philosophers of science than by scientists themselves). Researchers choose an existing theory. Then, they make a prediction about some new phenomenon that should be observed if the theory is correct. Again, this prediction is called a hypothesis. The researchers then conduct an empirical study to test the hypothesis. Finally, they reevaluate the theory in light of the new results and revise it if necessary.
This process is usually conceptualized as a cycle because the researchers can then derive a new hypothesis from the revised theory, conduct a new empirical study to test the hypothesis, and so on. As Figure 8.8 shows, this approach meshes nicely with the process of conducting a research project—creating a more detailed model of “theoretically motivated” or “theory-driven” research. Together, they form a model of theoretically motivated research.
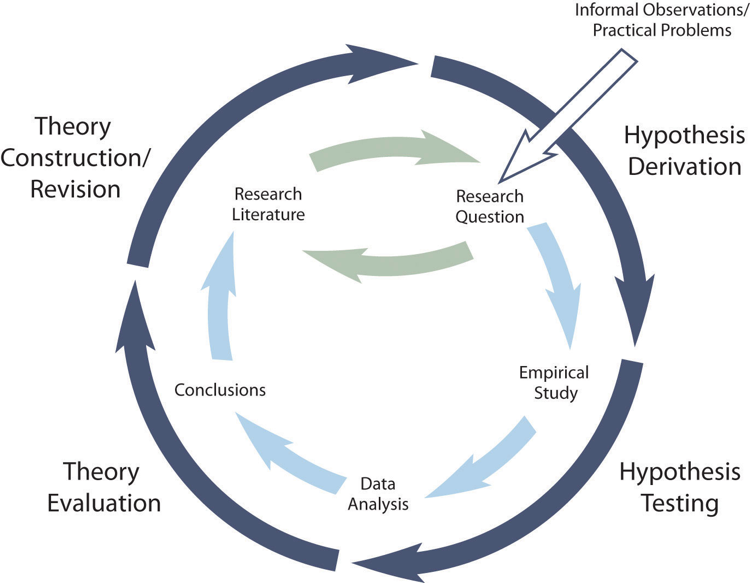
Keep in mind the hypothetico-deductive method is only one way of using social theory to inform social science research. It starts with describing one or more existing theories, deriving a hypothesis from one of those theories, testing your hypothesis in a new study, and finally reevaluating the theory based on the results data analyses. This format works well when there is an existing theory that addresses the research question—especially if the resulting hypothesis is surprising or conflicts with a hypothesis derived from a different theory.
But what if your research question is more interpretive? What if it is less about theory-testing and more about theory-building? This is what our next chapter covers: the process of inductively deriving theory from people’s stories and experiences. This process looks different than that depicted in Figure 8.8. It still starts with your research question and answering that question by conducting a research study. But instead of testing a hypothesis you created based on a theory, you will create a theory of your own that explain the data you collected. This format works well for qualitative research questions and for research questions that existing theories do not address.
Inductive reasoning is most commonly found in studies using qualitative methods, such as focus groups and interviews. Because inductive reasoning involves the creation of a new theory, researchers need very nuanced data on how the key concepts in their working question operate in the real world. Qualitative data is often drawn from lengthy interactions and observations with the individuals and phenomena under examination. For this reason, inductive reasoning is most often associated with qualitative methods, though it is used in both quantitative and qualitative research.
Whose truth does science establish?
Social work is concerned with the “isms” of oppression (ableism, ageism, cissexism, classism, heterosexism, racism, sexism, etc.), and so our approach to science must reconcile its history as both a tool of oppression and its exclusion of oppressed groups. Science grew out of the Enlightenment, a philosophical movement which applied reason and empirical analysis to understanding the world. While the Enlightenment brought forth tremendous achievements, the critiques of Marxian, feminist, and other critical theorists complicated the Enlightenment understanding of science. For this section, I will focus on feminist critiques of science, building upon an entry in the Stanford Encyclopedia of Philosophy (Crasnow, 2020). [16]
In its original formulation, science was an individualistic endeavor. As we learned in Chapter 1 , a basic statement of the scientific method is that a researcher studies existing theories on a topic, formulates a hypothesis about what might be true, and either confirms or disconfirms their hypothesis through experiment and rigorous observation. Over time, our theories become more accurate in their predictions and more comprehensive in their conclusions. Scientists put aside their preconceptions, look at the data, and build their theories based on objective rationality.
Yet, this cannot be perfectly true. Scientists are human, after all. As a profession historically dominated by white men, scientists have dismissed women and other minorities as being psychologically unfit for the scientific profession. While attitudes have improved, science, technology, engineering, mathematics (STEM) and related fields remain dominated by white men (Grogan, 2019). [17] Biases can persist in social work theory and research when social scientists do not have similar experiences to the populations they study.
Gender bias can influence the research questions scientists choose to answer. Feminist critiques of medical science drew attention to women’s health issues, spurring research and changing standards of care. The focus on domestic violence in the empirical literature can also be seen as a result of feminist critique. Thus, critical theory helps us critique what is on the agenda for science. If science is to answer important questions, it must speak to the concerns of all people. Through the democratization in access to scientific knowledge and the means to produce it, science becomes a sister process of social development and social justice.
The goal of a diverse and participatory scientific community lies in contrast to much of what we understand to be “proper” scientific knowledge. Many of the older, classic social science theories were developed based on research which observed males or from university students in the United States or other Western nations. How these observations were made, what questions were asked, and how the data were interpreted were shaped by the same oppressive forces that existed in broader society, a process that continues into the present. In psychology, the concept of hysteria or hysterical women was believed to be caused by a wandering womb (Tasca et al., 2012). [18] Even today, there are gender biases in diagnoses of histrionic personality disorder and racial biases in psychotic disorders (Klonsky et al., 2002) [19] because the theories underlying them were created in a sexist and racist culture. In these ways, science can reinforce the truth of the white Western male perspective.
Finally, it is important to note that social science research is often conducted on populations rather than with populations. Historically, this has often meant Western men traveling to other countries and seeking to understand other cultures through a Western lens. Lacking cultural humility and failing to engage stakeholders, ethnocentric research of this sort has led to the view of non-Western cultures as inferior. Moreover, the use of these populations as research subjects rather than co-equal participants in the research process privileges the researcher’s knowledge over that from other groups or cultures. Researchers working with indigenous cultures, in particular, had a destructive habit of conducting research for a short time and then leaving, without regard for the impact their study had on the population. These critiques of Western science aim to decolonize social science and dismantle the racist ideas the oppress indigenous and non-Western peoples through research (Smith, 2013). [20]
The central concept in feminist, anti-racist, and decolonization critiques (among other critical frames) is epistemic injustice. Epistemic injustice happens when someone is treated unfairly in their capacity to know something or describe their experience of the world. As described by Fricker (2011), [21] the injustice emerges from the dismissal of knowledge from oppressed groups, discrimination against oppressed groups in scientific communities, and the resulting gap between what scientists can make sense of from their experience and the experiences of people with less power who have lived experience of the topic. We recommend this video from Edinburgh Law School which applies epistemic injustice to studying public health emergencies, disabilities, and refugee services .

Positivism relies on nomothetic causality, or the idea that “one event, behavior, or belief will result in the occurrence of another, subsequent event, behavior, or belief.” Then, we described one kind of causality: a simple cause-and-effect relationship supported by existing theory and research on the topic, also known as a nomothetic causal relationship. But what if there is not a lot of literature on your topic? What if your question is more exploratory than explanatory? Then, you need a different kind of causal explanation, one that accounts for the complexity of human interactions.
How can we build causal relationships if we are just describing or exploring a topic? Recall the definitions of exploratory research , descriptive research , and explanatory research from Chapter 2. Wouldn’t we need to do explanatory research to build any kind of causal explanation? Explanatory research attempts to establish nomothetic causal relationships: an independent variable is demonstrated to cause change in a dependent variable. Exploratory and descriptive qualitative research contains some causal relationships, but they are actually descriptions of the causal relationships established by the study participants.
What do idiographic causal explanations look like?
An idiographic causal relationship tries to identify the many, interrelated causes that account for the phenomenon the researcher is investigating. So, if idiographic causal explanations do not look like Figure 8.5, 8.6, or 8.7 what do they look like? Instead of saying “x causes y,” your participants will describe their experiences with “x,” which they will tell you was caused and influenced by a variety of other factors, as interpreted through their unique perspective, time, and environment. As we stated before, idiographic causal explanations are messy. Your job as a social science researcher is to accurately describe the patterns in what your participants tell you.
Let’s think about this using an example. If I asked you why you decided to become a social worker, what might you say? For me, I would say that I wanted to be a mental health clinician since I was in high school. I was interested in how people thought, and I was privileged enough to have psychology courses at my local high school. I thought I wanted to be a psychologist, but at my second internship in my undergraduate program, my supervisors advised me to become a social worker because the license provided greater authority for independent practice and flexibility for career change. Once I found out social workers were like psychologists who also raised trouble about social justice, I was hooked.
That’s not a simple explanation at all! But it’s definitely a causal explanation. It is my individual, subjective truth of a complex process. If we were to ask multiple social workers the same question, we might find out that many social workers begin their careers based on factors like personal experience with a disability or social injustice, positive experiences with social workers, or a desire to help others. No one factor is the “most important factor,” like with nomothetic causal relationships. Instead, a complex web of factors, contingent on context, emerge when you interpret what people tell you about their lives.
Understanding “why?”
In creating an idiographic explanation, you are still asking “why?” But the answer is going to be more complex. Those complexities are described in Table 8.1 as well as this short video comparing nomothetic and idiographic relationships .
| Nomothetic causal relationships | Idiographic causal relationships | |
|---|---|---|
| Paradigm | Positivist | Interpretivist |
| Purpose of research | Prediction & generalization | Understanding & particularity |
| Reasoning | Deductive | Inductive |
| Purpose of research | Explanatory | Exploratory or descriptive |
| Research methods | Quantitative | Qualitative |
| Causality | Simple: cause and effect | Complex: context-dependent, sometimes circular or contradictory |
| Role of theory | Theory testing | Theory building |
Remember our question from the last section, “Are you trying to generalize or nah?” If you answered nah (or no, like a normal person), you are trying to establish an idiographic causal explanation. The purpose of that explanation isn’t to predict the future or generalize to larger populations, but to describe the here-and-now as it is experienced by individuals within small groups and communities. Idiographic explanations are focused less on what is generally experienced by all people but more on the particularities of what specific individuals in a unique time and place experience.
Researchers seeking idiographic causal relationships are not trying to generalize or predict, so they have no need to reduce phenomena to mathematics. In fact, only examining things that can be counted can rob a causal relationship of its meaning and context. Instead, the goal of idiographic causal relationships is understanding, rather than prediction. Idiographic causal relationships are formed by interpreting people’s stories and experiences. Usually, these are expressed through words. Not all qualitative studies use word data, as some can use interpretations of visual or performance art. However, the vast majority of qualitative studies do use word data, like the transcripts from interviews and focus groups or documents like journal entries or meeting notes. Your participants are the experts on their lives—much like in social work practice—and as in practice, people’s experiences are embedded in their cultural, historical, and environmental context.
Idiographic causal explanations are powerful because they can describe the complicated and interconnected nature of human life. Nomothetic causal explanations, by comparison, are simplistic. Think about if someone asked you why you wanted to be a social worker. Your story might include a couple of vignettes from your education and early employment. It might include personal experience with the social welfare system or family traditions. Maybe you decided on a whim to enroll in a social work course during your graduate program. The impact of each of these events on your career is unique to you.
Idiographic causal explanations are concerned with individual stories, their idiosyncrasies, and the patterns that emerge when you collect and analyze multiple people’s stories. This is the inductive reasoning we discussed at the beginning of this chapter. Often, idiographic causal explanations begin by collecting a lot of qualitative data, whether though interviews, focus groups, or looking at available documents or cultural artifacts. Next, the researcher looks for patterns in the data and arrives at a tentative theory for how the key ideas in people’s stories are causally related.
Unlike nomothetic causal relationships, there are no formal criteria (e.g., covariation) for establishing causality in idiographic causal relationships. In fact, some criteria like temporality and nonspuriousness may be violated. For example, if an adolescent client says, “It’s hard for me to tell whether my depression began before my drinking, but both got worse when I was expelled from my first high school,” they are recognizing that it may not so simple that one thing causes another. Sometimes, there is a reciprocal relationship where one variable (depression) impacts another (alcohol abuse), which then feeds back into the first variable (depression) and into other variables as well (school). Other criteria, such as covariation and plausibility, still make sense, as the relationships you highlight as part of your idiographic causal explanation should still be plausible and its elements should vary together.
Theory building and theory testing
As we learned in the previous section, nomothetic causal explanations are created by researchers applying deductive reasoning to their topic and creating hypotheses using social science theories. Much of what we think of as social science is based on this hypothetico-deductive method, but this leaves out the other half of the equation. Where do theories come from? Are they all just revisions of one another? How do any new ideas enter social science?
Through inductive reasoning and idiographic causal explanations!
Let’s consider a social work example. If you plan to study domestic and sexual violence, you will likely encounter the Power and Control Wheel, also known as the Duluth Model (Figure 8.9). The wheel is a model designed to depict the process of domestic violence. The wheel was developed based on qualitative focus groups conducted by sexual and domestic violence advocates in Duluth, MN. This video explains more about the Duluth Model of domestic abuse.

The Power and Control Wheel is an example of what an idiographic causal relationship looks like. By contrast, look back at the previous section’s Figure 8.5, 8.6, and 8.7 on nomothetic causal relationships between independent and dependent variables. See how much more complex idiographic causal explanations are?! They are complex, but not difficult to understand. At the center of domestic abuse is power and control, and while not every abuser would say that is what they were doing, that is the understanding of the survivors who informed this theoretical model. Their power and control is maintained through a variety of abusive tactics from social isolation to use of privilege to avoid consequences.
What about the role of hypotheses in idiographic causal explanations? In nomothetic causal explanations, researchers create hypotheses using existing theory and then test them for accuracy. Hypotheses in idiographic causality are much more tentative, and are probably best considered as “hunches” about what they think might be true. Importantly, they might indicate the researcher’s prior knowledge and biases before the project begins, but the goal of idiographic research is to let your participants guide you rather than existing social work knowledge. Continuing with our Duluth Model example, advocates likely had some tentative hypotheses about what was important in a relationship with domestic violence. After all, they worked with this population for years prior to the creation of the model. However, it was the stories of the participants in these focus groups that led the Power and Control Wheel explanation for domestic abuse.
As qualitative inquiry unfolds, hypotheses and hunches are likely to emerge and shift as researchers learn from what their participants share. Because the participants are the experts in idiographic causal relationships, a researcher should be open to emerging topics and shift their research questions and hypotheses accordingly. This is in contrast to hypotheses in quantitative research, which remain constant throughout the study and are shown to be true or false.
Over time, as more qualitative studies are done and patterns emerge across different studies and locations, more sophisticated theories emerge that explain phenomena across multiple contexts. Once a theory is developed from qualitative studies, a quantitative researcher can seek to test that theory. For example, a quantitative researcher may hypothesize that men who hold traditional gender roles are more likely to engage in domestic violence. That would make sense based on the Power and Control Wheel model, as the category of “using male privilege” speaks to this relationship. In this way, qualitatively-derived theory can inspire a hypothesis for a quantitative research project, as we will explore in the next section.
Complementary approaches
If idiographic and nomothetic still seem like obscure philosophy terms, let’s consider another example. Imagine you are working for a community-based non-profit agency serving people with disabilities. You are putting together a report to lobby the state government for additional funding for community support programs. As part of that lobbying, you are likely to rely on both nomothetic and idiographic causal relationships.
If you looked at nomothetic causal relationships, you might learn how previous studies have shown that, in general, community-based programs like yours are linked with better health and employment outcomes for people with disabilities. Nomothetic causal explanations seek to establish that community-based programs are better for everyone with disabilities, including people in your community.
If you looked at idiographic causal explanations, you would use stories and experiences of people in community-based programs. These individual stories are full of detail about the lived experience of being in a community-based program. You might use one story from a client in your lobbying campaign, so policymakers can understand the lived experience of what it’s like to be a person with a disability in this program. For example, a client who said “I feel at home when I’m at this agency because they treat me like a family member,” or “this is the agency that helped me get my first paycheck,” can communicate richer, more complex causal relationships.
Neither kind of causal explanation is better than the other. A decision to seek idiographic causal explanations means that you will attempt to explain or describe your phenomenon exhaustively, attending to cultural context and subjective interpretations. A decision to seek nomothetic causal explanations, on the other hand, means that you will try to explain what is true for everyone and predict what will be true in the future. In short, idiographic explanations have greater depth, and nomothetic explanations have greater breadth.
Most importantly, social workers understand the value of both approaches to understanding the social world. A social worker helping a client with substance abuse issues seeks idiographic explanations when they ask about that client’s life story, investigate their unique physical environment, or probe how their family relationships. At the same time, a social worker also uses nomothetic explanations to guide their interventions. Nomothetic explanations may help guide them to minimize risk factors and maximize protective factors or use an evidence-based therapy, relying on knowledge about what in general helps people with substance abuse issues.
So, which approach speaks to you? Are you interested in learning about (a) a few people’s experiences in a great deal of depth, or (b) a lot of people’s experiences more superficially, while also hoping your findings can be generalized to a greater number of people? The answer to this question will drive your research question and project. These approaches provide different types of information and both types are valuable.
- Idiographic causal explanations focus on subjectivity, context, and meaning.
- Idiographic causal explanations are best suited to exploratory research questions and qualitative methods.
- Idiographic causal explanations are used to create new theories in social science.
- Explore the literature on the theory you identified in section 8.1.
- Read about the origins of your theory. Who developed it and from what data?
- See if you can find a figure like Figure 8.9 in an article or book chapter that depicts the key concepts in your theory and how those concepts are related to one another causally. Write out a short statement on the causal relationships contained in the figure.
- List the key terms associated with qualitative research questions
- Distinguish between qualitative and quantitative research questions
Qualitative research questions differ from quantitative research questions. Because qualitative research questions seek to explore or describe phenomena, not provide a neat nomothetic explanation, they are often more general and openly worded. They may include only one concept, though many include more than one. Instead of asking how one variable causes changes in another, we are instead trying to understand the experiences , understandings , and meanings that people have about the concepts in our research question. These keywords often make an appearance in qualitative research questions.
Let’s work through an example from our last section. In Table 9.1, a student asked, “What is the relationship between sexual orientation or gender identity and homelessness for late adolescents in foster care?” In this question, it is pretty clear that the student believes that adolescents in foster care who identify as LGBTQ+ may be at greater risk for homelessness. This is a nomothetic causal relationship—LGBTQ+ status causes changes in homelessness.
However, what if the student were less interested in predicting homelessness based on LGBTQ+ status and more interested in understanding the stories of foster care youth who identify as LGBTQ+ and may be at risk for homelessness? In that case, the researcher would be building an idiographic causal explanation . The youths whom the researcher interviews may share stories of how their foster families, caseworkers, and others treated them. They may share stories about how they thought of their own sexuality or gender identity and how it changed over time. They may have different ideas about what it means to transition out of foster care.

Because qualitative questions usually center on idiographic causal relationships, they look different than quantitative questions. Table 9.3 below takes the final research questions from Table 9.1 and adapts them for qualitative research. The guidelines for research questions previously described in this chapter still apply, but there are some new elements to qualitative research questions that are not present in quantitative questions.
- Qualitative research questions often ask about lived experience, personal experience, understanding, meaning, and stories.
- Qualitative research questions may be more general and less specific.
- Qualitative research questions may also contain only one variable, rather than asking about relationships between multiple variables.
| How does witnessing domestic violence impact a child’s romantic relationships in adulthood? | How do people who witness domestic violence understand its effects on their current relationships? |
| What is the relationship between sexual orientation or gender identity and homelessness for late adolescents in foster care? | What is the experience of identifying as LGBTQ+ in the foster care system? |
| How does income inequality affect ambivalence in high-density urban areas? | What does racial ambivalence mean to residents of an urban neighborhood with high income inequality? |
| How does race impact rates of mental health diagnosis for children in foster care? | How do African-Americans experience seeking help for mental health concerns? |
Qualitative research questions have one final feature that distinguishes them from quantitative research questions: they can change over the course of a study. Qualitative research is a reflexive process, one in which the researcher adapts their approach based on what participants say and do. The researcher must constantly evaluate whether their question is important and relevant to the participants. As the researcher gains information from participants, it is normal for the focus of the inquiry to shift.
For example, a qualitative researcher may want to study how a new truancy rule impacts youth at risk of expulsion. However, after interviewing some of the youth in their community, a researcher might find that the rule is actually irrelevant to their behavior and thoughts. Instead, their participants will direct the discussion to their frustration with the school administrators or the lack of job opportunities in the area. This is a natural part of qualitative research, and it is normal for research questions and hypothesis to evolve based on information gleaned from participants.
However, this reflexivity and openness unacceptable in quantitative research for good reasons. Researchers using quantitative methods are testing a hypothesis, and if they could revise that hypothesis to match what they found, they could never be wrong! Indeed, an important component of open science and reproducability is the preregistration of a researcher’s hypotheses and data analysis plan in a central repository that can be verified and replicated by reviewers and other researchers. This interactive graphic from 538 shows how an unscrupulous research could come up with a hypothesis and theoretical explanation after collecting data by hunting for a combination of factors that results in a statistically significant relationship. This is an excellent example of how the positivist assumptions behind quantitative research and intepretivist assumptions behind qualitative research result in different approaches to social science.
- Qualitative research questions often contain words or phrases like “lived experience,” “personal experience,” “understanding,” “meaning,” and “stories.”
- Qualitative research questions can change and evolve over the course of the study.
- Using the guidance in this chapter, write a qualitative research question. You may want to use some of the keywords mentioned above.
- Kivuna, C. & Kuyini, A. B. (2017). Understanding and applying research paradigms in educational contexts. International Journal of Higher Education, 6 (5), 26-41. https://eric.ed.gov/?id=EJ1154775 ↵
- Kuhn, T. (1962). The structure of scientific revolutions . Chicago: University of Chicago Press. ↵
- Fleuridas, C., & Krafcik, D. (2019). Beyond four forces: The evolution of psychotherapy. Sage Open , 9 (1), 2158244018824492. ↵
- Shneider, A. M. (2009). Four stages of a scientific discipline; four types of scientist. Trends in Biochemical Sciences 34 (5), 217-233. https://doi.org/10.1016/j.tibs.2009.02.00 ↵
- Burrell, G. & Morgan, G. (1979). Sociological paradigms and organizational analysis . Routledge. Guba, E. (ed.) (1990). The paradigm dialog . SAGE. ↵
- Routledge. Guba, E. (ed.) (1990). The paradigm dialog . SAGE. ↵
- Burrell, G. & Morgan, G. (1979). Sociological paradigms and organizational analysis . Here is a summary of Burrell & Morgan from Babson College , and our classification collapses radical humanism and radical structuralism into the critical paradigm, following Guba and Lincoln's three-paradigm framework. We feel this approach is more parsimonious and easier for students to understand on an introductory level. ↵
- For more about how the meanings of hand gestures vary by region, you might read the following blog entry: Wong, W. (2007). The top 10 hand gestures you’d better get right . Retrieved from: http://www.languagetrainers.co.uk/blog/2007/09/24/top-10-hand-gestures ↵
- Rosario, M., Schrimshaw, E. W., Hunter, J., & Levy-Warren, A. (2009). The coming-out process of young lesbian and bisexual women: Are there butch/femme differences in sexual identity development?. Archives of sexual behavior , 38 (1), 34-49. ↵
- Calhoun, C., Gerteis, J., Moody, J., Pfaff, S., & Virk, I. (Eds.). (2007). Classical sociological theory (2nd ed.). Malden, MA: Blackwell. ↵
- Fraser, N. (1989). Unruly practices: Power, discourse, and gender in contemporary social theory . Minneapolis, MN: University of Minnesota Press. ↵
- Here are links to two HBSE open textbooks, if you are unfamiliar with social work theories and would like more background. https://uark.pressbooks.pub/hbse1/ and https://uark.pressbooks.pub/humanbehaviorandthesocialenvironment2/ ↵
- Box, G. E. P.. (1976). Science and statistics. Journal of the American Statistical Association, 71 (356), 791. ↵
- Heineman-Pieper, J., Tyson, K., & Pieper, M. H. (2002). Doing good science without sacrificing good values: Why the heuristic paradigm is the best choice for social work. Families in Society , 83 (1), 15-28. ↵
- Crasnow, S. (2020). Feminist perspectives on science. In E. N. Zalta (ed.), The Stanford Encyclopedia of Philosophy (Winter 2020 Edition). Retrieved from: https://plato.stanford.edu/entries/feminist-science/ ↵
- Grogan, K.E. (2019) How the entire scientific community can confront gender bias in the workplace. Nature Ecology & Evolution, 3 , 3–6. doi:10.1038/s41559-018-0747-4 ↵
- Tasca, C., Rapetti, M., Carta, M. G., & Fadda, B. (2012). Women and hysteria in the history of mental health. Clinical practice and epidemiology in mental health: Clinical practice & epidemiology in mental health , 8 , 110-119. ↵
- Klonsky, E. D., Jane, J. S., Turkheimer, E., & Oltmanns, T. F. (2002). Gender role and personality disorders. Journal of personality disorders , 16 (5), 464-476. ↵
- Smith, L. T. (2013). Decolonizing methodologies: Research and indigenous peoples . Zed Books Ltd. ↵
- Fricker, M. (2011). Epistemic injustice: Power and the ethics of knowing . Oxford University Press. ↵
The highest level of measurement. Denoted by mutually exclusive categories, a hierarchy (order), values can be added, subtracted, multiplied, and divided, and the presence of an absolute zero.
a paradigm based on the idea that social context and interaction frame our realities
a paradigm in social science research focused on power, inequality, and social change
a research paradigm that suspends questions of philosophical ‘truth’ and focuses more on how different philosophies, theories, and methods can be used strategically to resolve a problem or question within the researcher's unique context
A cyclical process of theory development, starting with an observed phenomenon, then developing or using a theory to make a specific prediction of what should happen if that theory is correct, testing that prediction, refining the theory in light of the findings, and using that refined theory to develop new hypotheses, and so on.
when someone is treated unfairly in their capacity to know something or describe their experience of the world
conducted during the early stages of a project, usually when a researcher wants to test the feasibility of conducting a more extensive study or if the topic has not been studied in the past
research that describes or defines a particular phenomenon
explains why particular phenomena work in the way that they do; answers “why” questions
attempts to explain or describe your phenomenon exhaustively, based on the subjective understandings of your participants
"Assuming that the null hypothesis is true and the study is repeated an infinite number times by drawing random samples from the same populations(s), less than 5% of these results will be more extreme than the current result" (Cassidy et al., 2019, p. 233).
Scientific Inquiry in Social Work (2nd Edition) Copyright © 2020 by Matthew DeCarlo, Cory Cummings, and Kate Agnelli is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License , except where otherwise noted.
Share This Book
Breadcrumbs Section. Click here to navigate to respective pages.

Working with Time in Qualitative Research
DOI link for Working with Time in Qualitative Research
Get Citation
This collection brings together researchers and scholars from across the Arts, Humanities and Social Sciences who are actively exploring the many different ways in which time might be understood, imagined and used in qualitative research. Taken together, the contributions begin to trace the contours of what it might mean to work reflexively with time as an epistemologically constitutive element of research design.
The book explores how the choice to work with pasts or futures, with speed or delay, with clocks or the time of the body, with utopias or failed futures (among other things) reframe how social and cultural phenomena are perceived and brought into existence in qualitative research. Drawing on fields as disparate as futures studies and history, literary analysis and urban design, utopian studies and science and technology studies, this collection serves as a resource for both new and experienced researchers in the humanities and social sciences. It is a critically important resource for beginning to explore the wide repertoire of theoretical and methodological tools for working with time in the research process.
The book also draws attention to the way that institutional research timescapes – from university workload patterns to funding processes and project timescales – themselves shape how and what it is possible to know in and about the world. It concludes with a rousing manifesto for scholars and researchers, proposing 10 key attributes of temporally reflexive research.
TABLE OF CONTENTS
Chapter | 18 pages, introduction, chapter 1 | 17 pages, the paris boulevard autrement, chapter 2 | 14 pages, chapter 3 | 17 pages, times of urgencies, chapter 4 | 19 pages, bringing the past back to life 1, chapter 5 | 17 pages, chapter 6 | 17 pages, paying attention to time in communication research, chapter 7 | 14 pages, doing time in social science and humanities research, chapter 8 | 17 pages, plagues, time, traumas and responsibilities 1, chapter 9 | 16 pages, the rhythms of research, chapter 10 | 15 pages, clocking invisible labour in academia, chapter 11 | 16 pages, working with/in time.
- Privacy Policy
- Terms & Conditions
- Cookie Policy
- Taylor & Francis Online
- Taylor & Francis Group
- Students/Researchers
- Librarians/Institutions
Connect with us
Registered in England & Wales No. 3099067 5 Howick Place | London | SW1P 1WG © 2024 Informa UK Limited
- Find My Rep
You are here

Case Study Methods
- Jacques Hamel - University of Montreal, Canada
- Stephane Dufour - University of Montreal, Canada
- Dominic Fortin - University of Montreal, Canada
- Description
Detailed text, more suited to PG level students and those wanting a more 'philosophical' text. This book was originally published in French. It is a thought provoking book, and worthy of extended reading, but not really suitable for many UG level students. I have certainly found it to be a book which outlines concepts and sets out the parameters and contexts for using case studies. Intriguing indeed!
For instructors
Select a purchasing option, order from:.
- VitalSource
- Amazon Kindle
- Google Play

SAGE Research Methods is a research methods tool created to help researchers, faculty and students with their research projects. SAGE Research Methods links over 175,000 pages of SAGE’s renowned book, journal and reference content with truly advanced search and discovery tools. Researchers can explore methods concepts to help them design research projects, understand particular methods or identify a new method, conduct their research, and write up their findings. Since SAGE Research Methods focuses on methodology rather than disciplines, it can be used across the social sciences, health sciences, and more.
With SAGE Research Methods, researchers can explore their chosen method across the depth and breadth of content, expanding or refining their search as needed; read online, print, or email full-text content; utilize suggested related methods and links to related authors from SAGE Research Methods' robust library and unique features; and even share their own collections of content through Methods Lists. SAGE Research Methods contains content from over 720 books, dictionaries, encyclopedias, and handbooks, the entire “Little Green Book,” and "Little Blue Book” series, two Major Works collating a selection of journal articles, and specially commissioned videos.
- Open access
- Published: 15 September 2024
Exploring academic and clinical nurses’ perspectives on evidence-based nursing course for undergraduates from perspectives of academic-practice partnerships: a qualitative study
- Guiyun Wang 1 ,
- Yuting Xia 2 ,
- Qirong Chen 2 ,
- Xirongguli Halili 2 &
- Hui Huang 3
BMC Nursing volume 23 , Article number: 657 ( 2024 ) Cite this article
Metrics details
To explore nurses’ perceptions of evidence-based nursing courses for undergraduates through academic-practice partnerships.
A deductive thematic analysis based on the practice-academic logic model.
Fifteen academic and clinical nurses were interviewed between November and December 2023, either online or through face-to-face meetings. Each interview lasted 20–30 min. The interview outline was constructed based on the practice-academic partnership logic model, which was followed during the process of recorded, analyzed, and checked.
Themes identified include inputs (e.g., stakeholder commitment), activities (e.g., communication), outputs (e.g., nursing projects), and outcomes (e.g., improved competence). These themes highlight the various aspects and outcomes of academic-practice partnerships in evidence-based nursing courses.
Effective academic-practice partnerships are crucial for developing evidence-based nursing courses, leading to positive educational and professional outcomes.
Nurses’ perceptions provide valuable guidelines for developing effective evidence-based nursing courses.
Patient or public contribution
No patient or public users participated in this study.
Peer Review reports
Introduction
Evidence-based nursing (EBN) is a systematic approach to addressing clinical questions that combines research findings, clinicians’ expertise, and patients’ values [ 1 ]. Conducting evidence-based nursing practices (EBNP) has a significant effect on improving the quality of nursing care and reducing healthcare expenses [ 2 , 3 , 4 ]. Over the past decade, researchers have emphasized the importance of EBNP [ 5 ]. However, limited EBNP projects has been conducted in clinical nursing [ 6 ]. The main reason for the insufficient implementation of EBNP is the lack of EBN knowledge, competence, resources, and adherence to complete processes and pathways by nurses [ 7 ]. Conducting high-quality EBN education is a key measure to improve the EBN competence of nurses [ 8 ]. Undergraduate nursing students are the future of the nursing workforce [ 9 , 10 ]. Undergraduate nursing students will have the competence to conduct EBNP projects to promote the development of nursing care towards a more professional and scientific direction [ 11 ]. American Medical Association has pointed out that conducting EBP education for undergraduate nursing students is the key to equipping them with EBN competence and enabling them to conduct EBNP [ 12 ].
Nevertheless, there is limited studies focused on developing of EBN education for undergraduate nursing students [ 11 ]. Existing studies have shown that EBN education for undergraduate nursing students mainly focuses on lectures, interactive, and blended online and offline teaching and the EBNP education for undergraduate nursing students were conducted by clinical nurses [ 12 , 13 , 14 ]. However, most of the clinical nurses lacked of time to provide systematic EBN theory education for undergraduate, which caused the undergraduate nursing student with low level of EBN knowledge and ability [ 13 , 14 , 15 , 16 , 17 ]. The separation of theory and practice is the main drawback of existing EBN education for undergraduate nursing students [ 13 , 14 ]. However, theory and practice are two essential and complementary components of EBN [ 18 ].
Academic-practice partnerships (APPs) refers to the establishment of strategic relationships between academic and clinical institutions, fully utilizing the advantages of both sides, and promoting common vision in teaching, practice, and research [ 19 ]. Conducting APPs in EBN (APPs-EBN) education will overcome the key obstacle of the existing EBN education for undergraduate nursing students [ 12 , 20 ]. To understand the content of APPs-EBN education, the steps of existing research of APPs-EBN training program for nursing students was shown as following [ 21 , 22 ]: (1) clinical nurses to identify their needs; (2) academic nurses assigned nursing students specific topics, provide reading materials and videos; (3) nursing students formulated EBNP questions (PICOs, including participants, interventions, comparison, outcomes, and study design [ 23 ]. PICOs were the important content of EBNP questions [ 23 ].); (4) academic nurses, clinical nurses and nursing students discussed the accuracy of EBNP questions (PICOs); (5) nursing students submitted their homework and received their grades with feedback; (6) academic and clinical nurses chose a final EBNP question (PICOs) that was befitting for each student group.
Academic nurses and clinical nurses should be the core of APPs-EBN education for undergraduate nursing students, actively participating in all stages of EBN education process [ 22 ]. Moreover, conducting APPs-EBN education must be achieved through individual-level partnerships of academic nurses and clinical nurses [ 20 , 24 ]. However, existing studies focused on discussing APPs-EBN practice at institutional level, with limited studies focused on the individual perspectives of APPs-EBN education, especially for the undergraduate nursing student’s EBN education [ 19 , 20 , 25 ]. Therefore, it is crucial to understand the perceptions of academic and clinical nurses on APPs-EBN course for undergraduate nursing students to provide information for improving the quality of APPs-EBN course for undergraduate nursing students. However, there is a lack of individual-level evidence on specific perceptions of APPs-EBN course for undergraduate nursing students.
Practice-academic partnership logic model was designed for APPs program. Given the efficacy of this model has been approved in the aspect of APPs and its appropriateness for this qualitative study to deductive specific and essential content during the process of APPs, further to provide basis for researchers conduct APPs-EBN course for undergraduate nursing students [ 22 ]. This model emphasizes that having specific inputs and conducting specific activities in the process of APPs may result in corresponding outputs and outcomes (inputs and activities → outputs and outcomes). Inputs encompass the necessary investments in the APPs-EBN education program, including partnership champions, compatible philosophies, common vision, key stakeholder commitment, formalized partnership agreement, shared goals and accountabilities and dedicated time and resources [ 22 , 26 ]. Activities involve specific actions or processes that must be undertaken to yield desired outcomes from the APPs, including open, ongoing communications, shared decision-making and professional development [ 22 , 26 ]. Outputs are the tangible and immediate deliverables stemming from the inputs and activities, including action plans and strategic plans [ 22 , 26 ]. Outcomes, both short-term and long-term, denote the changes or impacts that arise from the APPs, including successful completion of short-term (action plan) goals and successful completion of long-term (strategic) goals [ 22 , 26 ]. Therefore, this study aimed to explore and interpret the perceptions on APPs-EBN course for undergraduate nursing students among the academic nurses and clinical nurses based on the partnership-academic partnership logic model. This study will provide a valuable information for further constructing APPs-EBN course for undergraduate nursing students.
This qualitative study used deductive thematic analysis by using the practice-academic logic model [ 27 ]. The qualitative study was reported following the Consolidated Criteria for Reporting Qualitative Research checklist [ 28 ].
Participants
Considering that academic and clinical nurses were the main stakeholders in APPs-EBN course for undergraduate nursing students, this study conducted qualitative interviews with these two groups of people. Inclusion criteria for academic nurses was that academic nurses had experience in teaching EBN course for undergraduate and/or graduate nursing students. Inclusion criteria for clinical nurses were as follows: (1) clinical nurses were responsible for providing direct care to patients in a hospital unit. (2) clinical nurses have the experience in EBNP.
Data collection
The data were collected between November and December 2023. The interviews were conducted through online videoconferencing meetings or face-to-face meetings in participants’ offices. Each participant underwent a single interview session, with each interview lasting approximately 20–30 min. The interviews were conducted by the corresponding author (Y.X.) who was a female master’s nursing student and has completed qualitative research training.
The sampling method employed was purposive sampling, which can consciously select some participants who understand the research questions and provide rich information in the interviews [ 29 ]. The interview outline was constructed based on the practice-academic partnership logic model, which mainly includes what support did we need from both the organizational and individual levels to conduct APPs-EBN course for undergraduate nursing students? What activities could be conducted in APPs-EBN course to improve teaching effectiveness? What were the outputs of conducting APPs-EBN course for undergraduate nursing students? What were the outcomes for conducting APPs-EBN course for undergraduate nursing students?
Before conducting the formal interview, the researchers contacted the interviewees through WeChat (the social media most commonly used in China) to introduce the purpose, significance, and methods of this part of the research. After obtaining consent from the participants, the interview schedule was arranged to accommodate their availability. Before commencing the formal interviews, the researchers reiterated the research’s purpose, significance, and methodologies to the interviewees, while also ensuring the protection of their privacy. Detailed explanations were provided concerning the recording procedures, and the interviewees were requested to sign an informed consent form before the interviews officially commenced, including the recording process. The semi-structured interview outline served as a comprehensive guide throughout the interview process, ensuring that the interview content remained closely aligned with the research objectives. All the interviews were recorded. Any questions that arose during the interview were promptly addressed to maintain clarity and depth of the responses.
Data analysis
Within 24 h after the interview, two researchers (Y.X. and H.H) converted 15 interview recordings into written materials and listened to the recordings multiple times to ensure the accuracy of the transcription results. The interview transcriptions were analyzed in NVivo 12.0. The corresponding author (Y.X.) followed the following steps to code the perspectives of participants: immersing in the data, developing an initial thematic template, organizing the data based on the template, condensing data and reflecting, comparing and contrasting data within similar participant categories, and comparing and contrasting data with different participant categories [ 20 ]. After completing the initial encoding of all data, the corresponding author (Y.X.) shared and validated the encoding results with other members of the research team to form the final encoding result [ 30 ].
Ethic considerations
This study was approved by the Ethics Committee of a nursing school in Hunan Province in March 2023 (review number: E202313). All the recorded data are only used for this study and were backed up in an encrypted computer without Internet connection.
Nine academic nurses participated in this study, two males and seven females, with an average age of (38.00 ± 8.00) years. Among them, eight academic nurses have a doctoral degree, and one academic nurse has a master’s degree. The nine academic nurses were from five different school of nursing in China and both of them have the experience in participating the APP-EBN courses for nurses or graduate nursing students. Six clinical nurses participated in this study, all of them were females and have a master’s degree, with an average age of (37.17 ± 4.26) years. And six clinical nurses were from four different comprehensive hospital in China and three clinical nurses have the experience in participating the APP-EBN projects.
Four themes with 16 subthemes were generated based on practice-academic partnership logic model (Table 1 ), including inputs, activities, outputs, outcomes.
All participants considered the multilevel contents of inputs were the necessary investment of APPs-EBN course for undergraduate nursing students.
Key stakeholder commitment
A few participants noted that academic and clinical institutions needed to form formal partnership before developed APPs-EBN course for undergraduate nursing students, which was beneficial for promoting APPs-EBN course. As the opinion by one participant, “The first step of developing APPs-EBN course is to reach a consensus and sign a partnership agreement between academic and clinical leadership , and vigorously promote developing APPs-EBN course.” (Participant 14 , Clinical nurse) Developing a teaching team was one of the important aspects of achieving key stakeholder commitment of APPs. “How to attract clinical nurses to participate in the teaching team requires the academic and clinical institutions to sign some partnership agreements.” (Participant 2 , Academic nurse).
Key stakeholder commitment was an important input for developing APPs-EBN course for undergraduate nursing students and further promoting common interests in EBN education, practice, and research [ 31 ].
Shared mission
Some participants believed that shared mission was an important input for developing of APPs-EBN course for undergraduate nursing students. As a participant mentioned, “It is necessary to consider shared mission. For example , if the goal is to implement EBNP projects in clinical settings after the course , plans must be made to enhance these projects while developing the course.” (Participant 2 , Academic nurse) Academic and clinical institution had shared mission was conducive to making the partnerships process smoother [ 26 ]. For example, “The leadership is very important during the process of APPs. Leaderships of the academic and the nursing department of the clinical focus on a shared mission to develop this course , which may have a significant impact (on the development of APPs-EBN course for undergraduate nursing students).” (Participant 3 , Academic nurse) .
EBN training
Participants mentioned that EBN training was necessary for academic and clinical nurses to improve their EBN competence and acquire the newest knowledge about EBN.
“From organizational level , it is necessary to regularly provide EBNP training opportunities for clinical nurses or provide more updates and lectures on this EBN to academic nurses.” (Participant 3 , Academic nurse) . “If there is such specialized EBN training , it would be best for academic and clinical nurses to participate in systematic learning.” (Participant 5 , Academic nurse) . “Regular training for academic and clinical nurses is necessary. Academic nurses primarily participate in training programs related to EBNP and teaching ability , while clinical nurses primarily participate in training programs related to teaching ability.” (Participant 8 , Academic nurse) .
Developing and conducting APPs-EBN course for undergraduate nursing students required academic and clinical nurses to input a significant amount of time in communication and preparing for teaching APPs-EBN course.
“For some (academic and clinical) nurses , time may be the biggest problem , as building the APPs-EBN course requires partnerships between academic and clinical nurses , including spending time on partnership and individual lesson preparation.” (Participant 10 , Clinical nurse) . “It is difficult for clinical nurses to participant in teaching APPs-EBN course for undergraduate student during their own rest.” (Participant 7 , Academic nurse) . “Developing the APPs-EBN course demands a substantial investment of time from both academic and clinical nurses. From a clinical perspective , the success of this endeavor largely hinges on the level of support from nursing leaders. If nursing leaders truly value this course , they will ensure that clinical nurses have sufficient time to contribute to its teaching.” (Participant 14 , Clinical nurse) .
Instructional design
According to the characteristics of the target population (undergraduate nursing students), the development of APPs-EBN course instructional design (including learning objectives, learning contents, learning methods, and learning resources) was the cornerstone of developing and implementing EBN education [ 32 ]. “The learning objectives is actually your initial origin of instructional design. Firstly , it is necessary to analyze what abilities undergraduate nursing students need to possess in the future clinical nursing , what kind of foundation they need nurses (academic and clinical nurses) to lay for them during their learning period , and what kind of (EBN) knowledge and skills they need to be taught.” (Participant 9 , Academic nurse) .
Comprehensive and systematic educational resources form the foundation for promoting the acquisition of EBN knowledge among undergraduate nursing students [ 33 , 34 ]. Evidence retrieval is a crucial prerequisite for evidence implementation, and ample database resources can significantly enhance the teaching of evidence retrieval in APPs-EBN courses for these students [ 35 ]. Several participants highlighted that database resources are essential for developing APPs-EBN courses for undergraduate nursing students.
“Provide them (undergraduate nursing students) with database resources to access relevant databases for retrieval.” (Participant 8 , Academic nurse) . “Sometimes , we use databases from other universities , because our university actually doesn’t have any databases about evidence-based nursing. It is necessary for university to support more database resources.” (Participant 5 , Academic nurse) .
The participants stated that universities and hospitals provide incentives for academic and clinical nurses, which could enhance the teaching engagement of these professionals.
“The clinical nurses who participated in this course (APPs-EBN course for undergraduate nursing students) have some corresponding incentives , including establishing some educational reform projects and funding.” (Participant 5 , Academic nurse) . “Perhaps there should be time support and performance rewards for nurses (academic and clinical nurses) to participate in this course (APPs-EBN course for undergraduate nursing students). Especially for clinical nurses , they should be provided more time support and performance rewards and honors for the engagement in EBNP education.” (Participant 8 , Academic nurse) . “It is necessary that both the academic and clinical institutions provide clear incentives. If you participate in APPs-EBN course for undergraduate nursing students , it will be beneficial for evaluating professional titles. In addition , it is basic to provide academic and clinical teachers more salary.” (Participant 10 , Clinical nurse) .
Mutual trust
Mutual respect was a key condition for developing of APPs-EBN course for undergraduate nursing students [ 26 ]. As participants said that, “It is important to establish a good relationship between academic and clinical nurses , as well as to have some communication during the teaching process.” (Participant 1 , Academic nurse) “Academic and clinical nurses definitely need to fully respect each other’s suggestions and skills , which is actually a very important prerequisite for partnerships.” (Participant 9 , Academic nurse) .
Leadership support
Leadership support was an important input in developing of APPs-EBN course for undergraduate nursing students. Academic and clinical nurses participating in teaching were more familiar with the characteristics of nursing undergraduate students. The leadership of academic and clinical institutions should provide these professionals with greater rights in developing of APPs-EBN course. “Because this (APPs-EBN course) is intended for students (undergraduate nursing students). It is necessary for leaderships of academic and clinical institutions to provide them (academic and clinical nurses) full freedom to design or optimize this course on their own. ” (Participant 9 , Academic nurse) .
In addition, the time for participating in the teaching of APPs-EBN course the requires the leadership-level support. Leaders should provide academic and clinical nurses with more opportunities to conduct EBNP.
“The support of leaders is essential. For example , if undergraduate nursing students come to a hospital for internships , nursing leaders need to provide them with sufficient support to conduct EBNP projects or participate in the application of clinical guidelines.” (Participant 8 , Academic nurse) . “It is necessary to have the support of the nursing teaching and research department , as this department could identity clinical nurses (with EBNP experience). In addition , the support of nursing leaders is also very important , they could arrange the scheduling and teaching tasks for clinical nurses.” (Participant 15 , Clinical nurse) .
Participants considered activities were essential part during the process of developing of APPs-EBN course for undergraduate nursing student. The effective activities included ongoing communication and share decision-making.
Ongoing communication
Ongoing communications between academic and clinical teachers were beneficial for them to jointly develop and optimize the course, and clarified the teaching tasks of both sides.
“Academic and clinical nurses need to engage in lesson preparation collaboratively. While academic nurses may primarily teach theoretical courses , clinical nurses should work with them to monitor the course’s progress and integrate clinical questions into practical sessions. Both groups should discuss and coordinate to define the teaching tasks effectively.” (Participant 1 , Academic nurse) . “Academic and clinical nurses may need to discuss with both sides about how to better integrate the theory knowledge into the practical course. Firstly , partnership lesson preparation is a part of the teaching process in which both sides are aware of each other’s teaching tasks…… Some partnership discussions and feedback are also important.” (Participant 9 , Academic nurse) .
Share decision-making
Academic and clinical nurses shared decision-making to each other during the teaching process of APPs-EBN course for undergraduate nursing students, which was beneficial to APPs-EBN course for undergraduate nursing students [ 26 ]. For example, “Clinical nurses need to provide timely feedback to academic nurses on any suggestions they may have during the implementation of the course. Academic nurses should also observe if there are some problems that effect teaching quality that require optimization. In other words , adjustments need to be made through regular discussions and feedback between both sides , in order to optimize the course in a timely manner” (Participant 9 , Academic nurse) .
Participants described that APPs-EBN course for undergraduate nursing students may could form outputs.
EBNP projects
More EBNP projects could be conducted in the future. “In the future , academic and clinical nurses could establish partnerships channels , and more EBNP projects may generated.” (Participant 1 , Academic nurse) .
EBN manuals
EBN manuals may be the important output of APPs-EBN course for undergraduate nursing students. “If academic and clinical nurses collaborate to develop EBN course , they could create some manuals including case reports , teaching manuals or reference books to ensure teaching quality and homogeneity.” (Participant 5 , Academic nurse) .
Almost all the participants considered that six positive outcomes were short-term and long-term goals of APPs-EBN course for undergraduate nursing students.
Improved EBN awareness
Improving EBN awareness among undergraduate nursing students was a crucial learning objective of APPs-EBN course for undergraduate nursing students. As a participant mentioned, “Improving EBN awareness among undergraduate nursing students and ensuring they recognize its significance and value is crucial.” (Participant 9 , Academic nurse) .
Improving EBN awareness among undergraduate nursing students would be beneficial for them to conduct EBNP in future clinical nursing work. “They (undergraduate nursing students) should understand the process of EBN. For example , they know what the meaning of evidence transformation. When they work in clinical nursing , they may encounter some clinical problems. At that time , they could conduct evidence retrieval instead of judging just based on experience.” (Participant 7 , Academic nurse) .
Improved EBN competence
Undergraduate nursing students could master the basic knowledge and skills of EBP through participating in APPs-EBN course.
“Undergraduate nursing students are able to develop PICO questions for clinical questions and conduct evidence implementation projects.” (Participant 8 , Academic nurse) . “Through this course , students (undergraduate nursing students) will master some EBN basic knowledge and technical skills , and then be able to apply these methods and competences in practice.” (Participant 2 , Academic nurse) .
Increased EBN projects
The EBN knowledge and skills would be improved for undergraduate nursing students after participating in APPs-EBN course. Undergraduate nursing students may conduct more EBNP projects in clinical nursing in the future.
“They (nursing undergraduate students) will have the skills to conduct EBNP projects in the future , especially the project of evidence implementation. This is the EBNP skill they need to possess after working in clinical nursing in the future.” (Participant 9 , Academic nurse) . “The long-term goal is that undergraduate nursing students can conduct EBNP projects in clinical nursing in the future , and to improve their existing clinical nursing practices.” (Participant 5 , Academic nurse) .
Improved quality of nursing care
Participants considered that undergraduate nursing students would conduct EBNP projects in clinical nursing, which was beneficial for improving patient satisfaction and quality of nursing care.
“Maybe these (EBNP) projects will bring some benefits to patients and improve the quality of nursing care.” (Participant 9 , Academic nurse) . “In the long-term goal , it may be that undergraduate nursing students could apply the methods of EBN into clinical nursing in clinical nursing in the future. These results of EBNP projects may improve the quality of nursing care and patients’ satisfaction.” (Participant 6 , Academic nurse) .
Improved professional identity
Participants mentioned that undergraduate nursing students would have professional identity improvement after conducting EBNP projects. “After conducting EBNP projects , many of undergraduate nursing students actually have a sense of feedback and value. Therefore , it may also enhance their professional identity and their own sense of value” (Participant 9 , Academic nurse) .
This study aimed to explore the academic and clinical nurses’ perceptions on APPs-EBN course for undergraduate nursing students based on practice-academic partnership logic model. In this study, the specific contents of inputs, activities, outputs, and outcomes could further enriching the theoretical framework for developing APPs-EBN education and provide the details for developing of APPs-EBN course for undergraduate nursing students [ 22 ].
The specific content of inputs in this study validates and supplements the results of this scoping review (including key stakeholder commitment, shared mission, time, instructional design, mutual trust, leadership support) [ 22 ]. The results of this study indicated the significance of EBN training and incentives in facilitating the implementation of APPs-EBN course for undergraduate nursing students, which was similar with existing study conducted by Dr. Chen [ 20 ]. Notably, most academic nurses a lack of nursing care experience, leading to a limited understanding of specific process and challenges associated with EBNP projects [ 36 ]. Some clinical nurses a lack of theoretical knowledge of EBN, others were inadequately prepared to engage in teaching EBN courses [ 5 , 31 , 37 , 38 , 39 ], potentially impacting the learning outcomes of undergraduate nursing students participated in EBN courses [ 40 , 41 ]. Therefore, strengthening the training of academic nurses in EBNP and clinical nurses in EBN theoretical knowledge was crucial for improving their basic knowledge, competences, and teaching quality of EBN course.
Developing and conducting of an APPs-EBN course for undergraduate nursing students requires active participation from both academic and clinical nurses in the teaching of APPs-EBN course [ 31 , 42 ]. Sufficient incentives have promoting effect on the participation of academic and clinical nurses in the teaching of APPs-EBN course, which similar with the results of existing research [ 20 , 43 ]. Academic and clinical institutions should develop incentives such as professional title promotion and performance rewards for academic and clinical nurses to promote partnerships in developing and implementing APPs-EBN course for undergraduate nursing students. Effective incentives may help academic and clinical nurses overcome obstacles related to develop APPs-EBN course for undergraduate nursing students, such as lack of time [ 20 ].
The results of this study indicated that developing and conducting APPs-EBN course for undergraduate nursing students needed academic and clinical nurses conduct activities of ongoing communication and share decision making, which was consistent with the results of a scoping review [ 22 ]. Academic and clinical nurses participate in developing APPs-EBN course and conduct ongoing communication and shared decision making through meetings or group discussions during the stages of course planning, course commencement, and evaluation are crucial for refining APPs-EBN course [ 44 ]. Continuous activities between both sides can also promote partnerships between academic and clinical nurses, which may strengthen the connection between academic and clinical sides [ 20 ].
EBNP projects and EBN manuals were the outputs in this study, which was similar with the results of the EBNP quality improvement initiative from the perspective of APPs-EBN [ 45 ]. After conducting APPs-EBN course for undergraduate nursing students, academic and clinical nurses would establish stable cooperative relationships and more nursing undergraduate students have the awareness and ability to conduct EBNP projects. This may lead to more EBNP projects conducted by academic nurses, clinical nurses, and nursing undergraduate students in the future [ 20 ]. In addition, academic and clinical nurses could create EBN manuals related to APPs-EBN courses for undergraduate nursing students based on teaching experiences and insights gained from conducting this course. EBN manuals may provide a theoretical foundation, enabling more nursing schools domestically and internationally to conduct APPs-EBN course for undergraduate nursing students.
Conducting APPs-EBN course for undergraduate nursing students could yield various positive outcomes, aligning with the results of the scoping review [ 22 ]. Short-term goals of APPs-EBN course for undergraduate nursing students may include improved EBN awareness and improved EBN, as high-quality EBN education stands as a crucial measure to attain these goals [ 8 ]. Undergraduate nursing students who possess awareness of and competence in EBN are better prepared to incorporate EBN methodologies into nursing practice. This preparation is crucial for advancing long-term goals such as increasing EBN projects, enhancing the quality of nursing care, and strengthening professional identity [ 46 , 47 ]. Therefore, it is recommended that nursing educators to provide comprehensive inputs and actively participate in activities when conducting APPs-EBN course for undergraduate nursing students. This approach could lead to the generation of outputs and realization of desired outcomes.
Strength and limitation
The participants involved in this study came from four distinct regions in China, all of them with different educational features. This diversity contributes to the universality of the results of this study.
The limitation of this study was that not all participants have experience in APPs-EBN. This is primarily from the scarcity of nursing colleges in China providing EBN courses for undergraduate students. Consequently, it becomes challenging to recruit academic and clinical nurses with sufficient experience in APPs-EBN to participate in this study. In addition, all of the clinical nurses in this study have master’s degree, primarily because the study was conducted in China. Most nursing schools at various universities in China have developed EBN courses only for graduate students, while undergraduate nursing students typically do not receive systematic EBN course [ 48 ]. In the future, it would be beneficial to target recruitment towards both academic and clinical nurses with adequate experience in APPs-EBN and varying education levels for further interviews. This approach aims to garner additional insights and refine the theoretical framework and specific APPs-EBN course.
In addition, the interviews were conducted through online videoconferencing meetings or face-to-face meetings due to the limitations of time and space. For the online videoconferencing meeting, we turned on the camera during the online interview and recorded it with the informed consent of the participants. However, the continuity and fluency of the interview were affected to some certain extent due to network interruption.
Conclusions
Developing and conducting of APPs-EBN course for undergraduate nursing students involves investing inputs (Key stakeholder commitment, Shared mission, EBN training, Time, Instructional design, Incentive, Mutual trust, Leadership support) and conducting activities (Ongoing communication and Share decision-making) may lead to outputs (Educational resource) and outcomes (Improved EBN awareness, Improved EBN competence, Increased EBN projects, Improved quality of nursing care, Improved professional identity).
Data availability
All the original data were shown in the results section of the maunscript.
Melnyk BM, et al. Evidence-based Practice Culture and Mentorship Predict EBP implementation, nurse job satisfaction, and intent to stay: support for the ARCC(©) model. Worldviews Evid Based Nurs. 2021;18(4):272–81.
Article PubMed Google Scholar
Alqahtani N, et al. Nurses’ evidence-based practice knowledge, attitudes and implementation: a cross-sectional study. J Clin Nurs. 2020;29(1–2):274–83.
Dagne AH, et al. Implementation of evidence-based practice and associated factors among nurses and midwives working in Amhara Region government hospitals: a cross-sectional study. Reprod Health. 2021;18(1):36.
Article PubMed PubMed Central Google Scholar
Wu Y, et al. Do educational interventions aimed at nurses to support the implementation of evidence-based practice improve patient outcomes? A systematic review. Nurse Educ Today. 2018;70:109–14.
Yoo JY, et al. Clinical nurses’ beliefs, knowledge, organizational readiness and level of implementation of evidence-based practice: the first step to creating an evidence-based practice culture. PLoS ONE. 2019;14(12):e0226742.
Article CAS PubMed PubMed Central Google Scholar
Lv Y, Geng L, Zeng Y, Wang H. Qualitative study on the difficulties experienced by nursing managers during evidence-based nursing practice. J Nurs Sci (China). 2021;36(11):60–2. https://doi.org/10.3870/j.issn.1001-4152.2021.11.060 .
Article Google Scholar
Zhao J, et al. Evidence-based practice implementation in healthcare in China: a living scoping review. Lancet Reg Health West Pac. 2022;20:100355.
PubMed PubMed Central Google Scholar
González LMP, Fonseca DA, Bermeo RNZ. Evidence-based practice competences in nursing students at a university in Colombia. Nurse Educ Today. 2021;107:105094.
Hou R. (2013). The Construction of Access Indicator System of Undergraduate Nursing—Students’Clinical Teacher in Henan Province. (Master) Zhengzhou University (China).
Institute of Medicine Committee on the Robert Wood Johnson Foundation Initiative on. The future of nursing, a.t.I.o.M. The future of nursing: leading change, advancing Health. National Academies Press (US); 2011.
Mthiyane GN, Habedi DS. The experiences of nurse educators in implementing evidence-based practice in teaching and learning. Health SA. 2018;23:1177.
Xu J, Guan Y, Shi H, Zhang Y, Zheng J, Wu C. Evidence-based practice education in undergraduate nursing students: a scoping review. Chin Jouranl Nurs Educ (China). 2022;19(3):277–83. https://doi.org/10.3761/j.issn.1672-9234.2022.03.01613 .
Keib CN, et al. Changes in nursing students’ perceptions of research and evidence-based practice after completing a research course. Nurse Educ Today. 2017;54:37–43.
Kim JS, Gu MO, Chang H. Effects of an evidence-based practice education program using multifaceted interventions: a quasi-experimental study with undergraduate nursing students. BMC Med Educ. 2019;19(1):71.
Cardoso D et al. The Effectiveness of an Evidence-Based Practice (EBP) Educational Program on Undergraduate Nursing Students’ EBP Knowledge and Skills: A Cluster Randomized Control Trial. Int J Environ Res Public Health, 2021. 18(1).
Rholdon R, et al. An embedded EBP project: Effect on student nurses’ practice, attitude, and knowledge. Teach Learn Nurs. 2021;16(2):110–5.
Chen Q et al. Differences in evidence-based nursing practice competencies of clinical and academic nurses in China and opportunities for complementary collaborations: a cross-sectional study. J Clin Nurs, 2022.
Ramis MA, et al. Theory-based strategies for teaching evidence-based practice to undergraduate health students: a systematic review. BMC Med Educ. 2019;19(1):267.
Beal JA. Academic-service partnerships in nursing: an integrative review Nurs Res Pract, 2012. 2012: p. 501564.
Chen Q et al. Academic and Clinical Nurses’ Perceptions and Experiences on Academic-Practice Partnership in Evidence-Based Practice: An Interpretive Description Journal of Nursing Management, 2023. 2023.
McClinton TD. A guided search: formulating a PICOT from assigned areas of inquiry. Volume 19. WORLDVIEWS ON EVIDENCE-BASED NURSING; 2022. pp. 426–7. 5.
Xia Y, et al. Academic-practice partnerships in evidence-based nursing education: a theory-guided scoping review. Nurse Educ Pract. 2023;73:103839.
Zhao Q, et al. Non-pharmacological interventions to prevent and treat delirium in older people: an overview of systematic reviews. Int J Nurs Stud. 2023;148:104584.
Rycroft-Malone J, et al. Collaboration and co-production of knowledge in Healthcare: opportunities and challenges. Int J Health Policy Manag. 2016;5(4):221–3.
De Geest S, et al. Academic service partnerships: what do we learn from around the globe? A systematic literature review. Nurs Outlook. 2013;61(6):447–57.
MacPhee M. Developing a practice-academic partnership logic model. Nurs Outlook. 2009;57(3):143–7.
Blum ER, Stenfors T, Palmgren PJ. Benefits of massive Open Online Course participation: deductive thematic analysis. J Med Internet Res. 2020;22(7):e17318.
Buus N, Perron A. The quality of quality criteria: replicating the development of the Consolidated Criteria for Reporting Qualitative Research (COREQ). Int J Nurs Stud. 2020;102:103452.
Su JJ, et al. Defining compassionate nursing care. Nurs Ethics. 2020;27(2):480–93.
Lasater K, Atherton IM, Kyle RG. Population health as a ‘platform’ for nurse education: a qualitative study of nursing leaders. Nurse Educ Today. 2020;86:104313.
Pedregosa S, et al. Effective academic-practice partnership models in nursing students’ clinical placement: a systematic literature review. Nurse Educ Today. 2020;95:104582.
Sukkarieh-Haraty O, Hoffart N. Integrating evidence-based practice into a Lebanese nursing baccalaureate program: challenges and successes. Int J Nurs Educ Scholarsh, 2017. 14(1).
Li S, Cao M, Zhu X. Evidence-based practice: knowledge, attitudes, implementation, facilitators, and barriers among community nurses-systematic review. Med (Baltim). 2019;98(39):e17209.
Wakibi S et al. Teaching evidence-based nursing practice to student nurses in developing countries: strategies for novice nurse educators. Int J Nurs Educ Scholarsh, 2020. 17(1).
Alving BE, Christensen JB, Thrysøe L. Hospital nurses’ information retrieval behaviours in relation to evidence based nursing: a literature review. Health Info Libr J. 2018;35(1):3–23.
Orta R, et al. Knowledge and competency of nursing Faculty regarding evidence-based practice. J Contin Educ Nurs. 2016;47(9):409–19.
Saunders H, et al. Practicing Healthcare professionals’ evidence-based practice competencies: an overview of systematic reviews. Worldviews Evid Based Nurs. 2019;16(3):176–85.
Camargo FC, et al. Competences and barriers for the evidence-based practice in nursing: an integrative review. Rev Bras Enferm. 2018;71(4):2030–8.
Cleary-Holdforth J. Evidence-based practice in nursing and midwifery: we are talking the talk, but are we walking the Walk? Worldviews Evid Based Nurs. 2020;17(2):94–7.
Lam CK, Schubert CF, Herron EK. Evidence-based practice competence in nursing students preparing to transition to practice. Worldviews Evid Based Nurs. 2020;17(6):418–26.
Lam CK, Schubert C. Evidence-based practice competence in nursing students: an exploratory study with important implications for educators. Worldviews Evid Based Nurs. 2019;16(2):161–8.
Gilliss CL, et al. Academic/clinical nursing integration in academic health systems. Nurs Outlook. 2021;69(2):234–42.
Speroni KG, McLaughlin MK, Friesen MA. Use of evidence-based Practice Models and Research Findings in Magnet-designated hospitals across the United States: National Survey results. Worldviews Evid Based Nurs. 2020;17(2):98–107.
Amaral C, et al. Patient Safety Training Programs for Health Care professionals: a scoping review. J Patient Saf. 2023;19(1):48–58.
PubMed Google Scholar
Otts JA, et al. Academic-practice Partnership to prevent and manage pressure injuries: an evidence-based Quality Improvement Initiative. J Wound Ostomy Cont Nurs. 2023;50(6):463–73.
Fu L, et al. Evidence-based practice competency and related factors among nurses working in Public hospitals. Inquiry. 2020;57:46958020927876.
André B, Aune AG, Brænd JA. Embedding evidence-based practice among nursing undergraduates: results from a pilot study. Nurse Educ Pract. 2016;18:30–5.
Jiao Y. Study on the status quo of evidence-based nursing quality of clinical undergraduate nurses and the construction of training contents (Master). Shanxi Medical University (China); 2017.
Download references
Acknowledgements
Not Application.
This work was supported by the Natural Science Foundation of Hunan Province (No.2022JJ40642) and the National Natural Science Foundation of China (No. 72104250).
Author information
Authors and affiliations.
School of Nursing, Shandong Xiehe University, Jinan, China
Guiyun Wang
Xiangya School of Nursing, Central South University, Changsha, China
Yuting Xia, Qirong Chen & Xirongguli Halili
The Third Xiangya Hospital, Central South University, Changsha, China
You can also search for this author in PubMed Google Scholar
Contributions
Study design: YX, HH, QC; Literature searching: YX, XH; Quality Appraisal: YX, HH, QC; Data extraction: YX, GW, QC; Study supervision: QC, GW, HH; Manuscript drafting: YX; Critical revisions for important intellectual content: YX, QC, HH, GW.
Corresponding authors
Correspondence to Yuting Xia or Hui Huang .
Ethics declarations
Ethics approval and consent to participate.
This study was approved by the Ethics Committee of school of nursing of Central South university, China (review number: E202313). Detailed explanations were provided concerning the recording procedures, and the interviewees were requested to sign an informed consent form before the interviews officially commenced, including the recording process.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/ .
Reprints and permissions
About this article
Cite this article.
Wang, G., Xia, Y., Chen, Q. et al. Exploring academic and clinical nurses’ perspectives on evidence-based nursing course for undergraduates from perspectives of academic-practice partnerships: a qualitative study. BMC Nurs 23 , 657 (2024). https://doi.org/10.1186/s12912-024-02223-1
Download citation
Received : 16 April 2024
Accepted : 02 August 2024
Published : 15 September 2024
DOI : https://doi.org/10.1186/s12912-024-02223-1
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Academic-practice partnerships
- Evidence-based nursing
- Undergraduate nursing students
- Perceptions
BMC Nursing
ISSN: 1472-6955
- General enquiries: [email protected]
Exploring preparedness transitions in medicine and pharmacy: a qualitative longitudinal study to inform multiprofessional learning opportunities
- Open access
- Published: 16 September 2024
Cite this article
You have full access to this open access article

- Ella Ottrey 1 ,
- Charlotte E. Rees 1 , 2 ,
- Caitlin Kemp 1 ,
- Kayley M. Lyons 3 , 4 ,
- Tina P. Brock 3 , 5 ,
- Michelle Leech 6 ,
- Lynn V. Monrouxe 7 &
- Claire Palermo 1
Despite extensive preparedness literature, existing studies fail to adequately explore healthcare graduates’ feelings of preparedness longitudinally across new graduate transition journeys, nor do they compare different healthcare professions to ascertain what opportunities exist for multiprofessional transition interventions. Therefore, this Australian study, underpinned by temporal theory, explores the preparedness transitions of medicine and pharmacy graduates. Our 6-month qualitative longitudinal study involved 12 medicine and 7 pharmacy learners after purposive sampling. They participated in an entrance interview before starting internship, longitudinal audio-diaries during their first three months of internship, and an exit interview. Framework analysis explored patterns in the data cross-sectionally and longitudinally for the whole cohort (thinking over time), with pen portraits illustrating individuals’ journeys (thinking through time). Preparedness and unpreparedness narratives involved practical skills and tasks, interpersonal skills, knowledge, and professional practice for medicine and pharmacy. However, narratives for practical skills and tasks, and professional practice were dominant amongst medicine graduates, while narratives for interpersonal skills and knowledge were dominant amongst pharmacy graduates. We found numerous cohort changes in feelings of preparedness over time, but the illustrative pen portraits demonstrated the complexities and nuances through time, including feelings of preparedness before internship becoming unpreparedness during internship (e.g., cannulas), improving preparedness through time (e.g., cover shifts), and persistent feelings of unpreparedness (e.g., patient interactions). While our cross-sectional findings are reasonably consistent with existing research, our comparative and longitudinal findings are novel. We recommend that educators build learners’ preparedness through uniprofessional transition interventions involving practical skills and tasks, and professional practice in medicine, and interpersonal skills and knowledge in pharmacy. More importantly, we recommend multiprofessional transition interventions for medicine and pharmacy learners before internship focusing on knowledge, and during internship focusing on practical skills and tasks.
Similar content being viewed by others
At the precipice: a prospective exploration of medical students’ expectations of the pre-clerkship to clerkship transition.

Endured and prevailed: a phenomenological study of doctors’ first year of clinical practice

A phenomenological study of new doctors’ transition to practice, utilising participant-voiced poetry
Explore related subjects.
- Medical Ethics
- Artificial Intelligence
Avoid common mistakes on your manuscript.
Introduction
Preparedness for practice matters in healthcare. It matters to new graduates as they navigate exciting and daunting transitions into the world of healthcare work, with its associated responsibilities and identities. It matters to new graduates’ colleagues as they simultaneously rely on their contributions to the healthcare team, and serve to support, mentor, and manage these novice colleagues. And perhaps most importantly, preparedness matters to patients and their significant others, who expect to be treated with safety, dignity, and competence by new graduates. Therefore, considerable literature already exists outlining what healthcare graduates feel prepared or unprepared for. However, to date, this literature is largely uniprofessional and cross-sectional, meaning that crucial gaps remain in healthcare educators’ knowledge about the similarities and differences in preparedness between professions, and how preparedness changes through time. As such, educators may not fully realise the opportunities to develop multiprofessional transition to practice interventions, nor identify the ideal content and timing for these interventions. Therefore, this novel study extends the burgeoning preparedness literature by exploring comparatively graduates’ feelings of preparedness longitudinally across their final year student-new graduate transitions in medicine and pharmacy. This work enables us to provide recommendations for uniprofessional and multiprofessional transition interventions across new graduates’ journeys into and through internship.
Preparedness across healthcare professions
Interestingly, preparedness has been conceptualised in multiple ways in the literature including experience, knowledge, confidence, resilience, short-term, and so on (Brennan et al., 2024 ; Ottrey et al., 2021 ). Considerable cross-sectional literature exists outlining the preparedness of uniprofessional groups for practice. A recent literature review revealed that 70–80% of medical graduates report feeling adequately prepared, but this was task-dependent (Padley et al., 2021 ). Regarding pharmacy interns, studies have reported diversity in preparedness for practice (see Table 1 ). A handful of studies have explored preparedness (sometimes focusing on preparedness for interprofessional practice) in final year students or new graduates from multidisciplinary groups, including: medicine, dentistry, nursing and/or midwifery, and/or allied health (Brennan et al., 2024 ; Ebert et al., 2014 ; Malau-Aduli et al., 2022 ; Merga, 2016 ; Walker et al., 2013 ). Together, these studies illustrate that final year students or new graduates are generally prepared for patient-centred practice, history-taking, examining patients, basic clinical skills, using guidelines, promoting patient safety and hygiene, and seeking support (Malau-Aduli et al., 2022 ; Walker et al., 2013 ). However, they illustrate under-preparedness for communicating with diverse people, clinical reasoning, prescribing, providing nutrition care, interprofessional teamworking, managing interpersonal conflict, recognising when to seek support, ward-specific knowledge, awareness of hospital policies and procedures, caseload and time management, clinical administration skills (e.g., audit, informatics, governance), high-risk patients and emergencies, applying theoretical knowledge to practice, teaching, coping with uncertainty, and stress management (Ebert et al., 2014 ; Malau-Aduli et al., 2022 ; Merga, 2016 ; Walker et al., 2013 ). On balance, preparedness for practice appeared similar across diverse professions, although some studies have started to illuminate differences (e.g., nursing graduates struggled to seek support and apply theory to practice, but medical graduates did not: Merga, 2016 ; Walker et al., 2013 ; Brennan et al., 2024 ). While these cross-sectional studies help to shed important light on healthcare graduates’ preparedness, numerous scholars have called for longitudinal research to further advance this important topic (e.g., Malau-Aduli et al., 2022 ; Monrouxe et al., 2017 , 2018 ; Sumpradit et al., 2014 ). However, few longitudinal studies exist to date (Padley et al., 2021 ), and several only report cross-sectional findings (e.g., Lefroy et al., 2017 ; Monrouxe et al., 2018 ).
Temporal theory: preparedness across healthcare professions through and over time
Time is central to qualitative longitudinal research (QLR: Neale, 2018 , 2019 ), and can be conceptualised in various ways (Rees & Ottrey, in press). In health-related QLR, time is often conceptualised as change, process, transition, and development (Audulv et al., 2022 ). Perhaps most relevant to the current study, time can be conceptualised as subjective, fluid and dynamic (i.e., thinking through time) or objective, linear and fixed (i.e., thinking over time: Audulv et al., 2022 ; Balmer & Richards, 2022 ; Balmer et al., 2021 ). Indeed, thinking through time enables researchers to focus on analysing experiences throughout a journey, including: “the stops and starts, detours, transitions and reversals of students’ progression” (Balmer et al., 2021 , p. 1254). Conversely, thinking over time enables researchers to compare experiences at multiple timepoints, such as the start and end of rotations. Embedded within this fixed/fluid conceptualisation, time can also be considered as a snapshot in time or unfolding through time (called synchronic and diachronic respectively: Neale, 2018 , 2019 ). Furthermore, researchers can orientate themselves to time across multiple planes including: (a) past, present and/or future (prospective-retrospective); and (b) short or long-term (intensive-extensive: Audulv et al., 2022 ; Balmer et al., 2021 ; Neale, 2018 , 2019 ).
Four longitudinal studies have explored medical or pharmacy graduates’ preparedness temporally: either through or over time. Viewing time as fluid, Monrouxe et al. ( 2014 ) conducted a longitudinal audio-diary (LAD) study exploring medical graduates’ preparedness through time. However, three longitudinal questionnaire studies explored preparedness in medical or pharmacy graduates over time, viewing time as fixed (Chaou et al., 2021 ; Chow et al., 2022 ; Mak et al., 2013 ). These four studies demonstrate general improvements in competence and confidence across time, such as for history-taking, physical examinations, clinical reasoning, and communication (Chaou et al., 2021 ; Chow et al., 2022 ; Mak et al., 2013 ; Monrouxe et al., 2014 ). However, these studies also illustrate ongoing unpreparedness (e.g., for end-of-life care, mental state examinations, and respiratory function tests) despite transition interventions (Chow et al., 2022 ), and challenging circumstances generating feelings of unpreparedness for aspects that graduates had previously felt prepared for (e.g., being on-call, interprofessional teamworking, patient management, and self-directed learning: Chaou et al., 2021 ; Monrouxe et al., 2014 ). Finally, some cross-sectional and retrospective studies involving medical graduates have reported improvements in preparedness over time, such as responding to acutely unwell patients, carrying out clinical procedures, and coping with new clinical situations (Burridge et al., 2020 ; Walker et al., 2013 ).
Critique of literature and study aim
The primary research outlined above typically involved descriptive, cross-sectional questionnaire surveys with uniprofessional graduates or educators. Some studies employed interviews with graduates or educators at one timepoint. The few multiprofessional studies conducted were also typically cross-sectional descriptive studies employing surveys or interviews/focus groups, and explored preparedness/readiness for clinical practice, including interprofessional practice. Additional criticisms include small sample (or sub-group) sizes and/or low response rates for questionnaires. Uniprofessional studies make it hard to understand the similarities and differences between new graduates’ preparedness, and thus what opportunities exist to develop multiprofessional transition interventions. Cross-sectional studies make it challenging to know how preparedness changes through time, and thus when multiprofessional transition interventions should be optimally timed. Therefore, this study—part of a broader research program on new graduate transitions amongst learners from dietetics, medicine, nursing, and pharmacy (Blair et al., 2023 ; Ottrey et al., 2021 ; Rees et al., 2022 )—aims to explore medicine and pharmacy learners’ feelings of preparedness during their final year student-new graduate transition journeys (i.e., the months after graduation) to better understand what opportunities might exist for multiprofessional transition interventions. We sought to answer two research questions (RQs) based on temporal theory:
RQ1: What are the key areas of perceived preparedness and unpreparedness for medicine and pharmacy graduates, and how do they compare between the professions?
RQ2: How do feelings of preparedness change over and through the final year student-new graduate transition, and how do they compare between medicine and pharmacy graduates?
Study design and grand theories.
This Australian study employs QLR (Neale, 2018 ; Neale & Flowerdew, 2003 ; SmithBattle et al., 2018 ; Vogl et al., 2018 ), grounded in social constructionism, valuing diversity in experiences and the construction of knowledge through social interaction (Burr, 2015 ; Rees et al., 2020 ). Indeed, our QLR was based on interpretivist philosophies privileging relativist ontology, subjectivist epistemology, and temporality of participants’ experiences. Our study design aligns with conceptualisations of time as fixed and fluid, synchronic and diachronic, prospective and retrospective, micro (i.e., individuals/small collectives), and intensive (i.e., short-term: Audulv et al., 2022 ; Balmer et al., 2021 ; Neale, 2018 , 2019 ; Rees & Ottrey, in press). We elicited stories about preparedness from participants across three phases: (1) entrance interviews around degree completion before starting internship, (2) longitudinal audio-diaries (LADs) through a 3-month period entering the workforce as interns, and (3) exit interviews (Gordon et al., 2017 , 2020 ; Monrouxe, 2009 ). See Fig. 1 for a visual representation of the data collection methods and their timing.

Visual representation of the data collection methods and their timing
At the time of the study, this undergraduate medical degree, accredited by the Australian Medical Council, was a five-year program; with two pre-clinical years, followed by three years with approximately 560 days of hospital and community-based clinical placements (with Year 5 predominantly in hospitals). Most students began the program in Year 1, but approximately 25% took graduate entry into Year 2 (after completing biomedicine, science, physiotherapy, or pharmacy degrees). The learning modes were varied (i.e., lectures, seminars, workshops, tutorials, and simulation sessions), with interprofessional activities (with nursing and midwifery, nutrition science, and radiation science students) embedded in curriculum and assessment activities throughout the program. Transition interventions designed to support preparation for practice in Year 5 included ‘back to base’ days every 4–6 weeks and a ‘back to base’ week just prior to graduation. Medicine graduates then entered a paid internship year at an approved hospital with provisional registration. At the time of the study, internship involved five 10-week rotations through medicine, emergency medicine, surgery, and other specialties (e.g., mental health, neurology/stroke, palliative care), at metropolitan and/or rural/regional hospitals. After students submitted their rotation preferences, internships were coordinated through the Postgraduate Medical Council of Victoria. At the time of the study, this undergraduate pharmacy degree was comprised of four (predominantly pre-clinical) years accredited by the Australian Pharmacy Council. While most students began the program in Year 1, graduate entry into Year 3 was offered to those with science or biomedical science degrees. The teaching models were predominately lectures, tutorials and laboratory activities, with course content focusing primarily on foundational sciences. Students completed 60 days of professional experiential placement across Years 3 and 4. No specific multi- or interprofessional training or substantial transition interventions were included. Pharmacy graduates entered a one-year paid (clinical) internship program, operated by the university or another accredited internship provider (e.g., professional society), and undertaken at community pharmacies or in hospitals. At the time of the study, internship involved 1824 h of supervised practice, and could include rotations of various lengths through different settings (e.g., hospital dispensary, wards), in addition to assessments, workshops, and training sessions ahead of the Pharmacy Board examination. Both medicine and pharmacy interns secured full registration via the Australian Health Practitioner Regulation Agency on successful completion of their intern year.
Sampling and recruitment
After securing ethics approval, we used purposive (i.e., maximum variation) sampling to recruit diverse final year students from four professions at an Australian university (Kitto et al., 2008 ). We wanted diversity in terms of students’ demographics (i.e., gender, ethnicity, and age), as well as professional affiliations (i.e., dietetics, medicine, nursing, and pharmacy). This paper focuses on medicine and pharmacy graduates only because: (a) both have provisional registration granted after graduation with full registration after successfully completing a 12-month internship; and (b) the increased task shifting and scope of practice for pharmacy (e.g., prescribing, vaccinating). We employed different recruitment methods, including email and in-person invitations, and snowballing. Our temporal sampling of final year students (before and during their early experiences of work as interns typically within hospitals but sometimes in a community setting) allowed us to track preparedness views and experiences through the university to workforce transition across a 6-month period. In total, 19 final year students participated in phases 1 and 2 (12 medicine, 7 pharmacy), with reasonable retention into phase 3 (15 participants: 9 medicine, 6 pharmacy). See Online Supplementary Table for a summary of participants’ involvement across the study. At the study outset, participants were predominately female (n = 16, 84%) and of Oceanian descent (n = 12, 63%; as defined by the Australian Bureau of Statistics, including Australian Peoples), with a median age of 23 years. Further participant demographics are reported elsewhere (Blair et al., 2023 ; Ottrey et al., 2021 ; Rees et al., 2022 ).
Data collection
In the first phase, entrance interviews, we spoke to 19 participants in eight group interviews (5 medicine groups, 3 pharmacy groups; purposefully grouping participants by discipline) (Oct–Dec 2019). All interviews were conducted in-person and audio-recorded. Participants completed a personal details questionnaire. Then, led by a discussion guide to promote consistency between interviewers (CK, KML, EO), we asked participants to tell us what they thought about ‘preparedness for practice’ (Ottrey et al., 2021 ) and ‘transition’ (Rees et al., 2022 ). Employing narrative interviewing techniques (Riessman, 2008 ), we invited participants to share memorable stories of times when they felt prepared and unprepared for practice in their final year of study (see Appendix 1 ). When needed, we prompted for further information, such as when and where the scenario happened. Afterwards, we briefed participants on the second phase and invited their participation. Entrance interviews lasted on average 72 min (range 58–88), generating 9 h and 31 min of data.
All 19 participants (100%) took part in the second phase, where we used longitudinal audio-diaries (LADs) to gather preparedness stories weekly through a 3-month period during Dec 2019–Mar 2020 (Monrouxe, 2009 ). We provided a LAD guide, which prompted topics such as preparedness or unpreparedness experiences from that week, and their impacts (see Appendix 1 ). The LAD guide encouraged participants to share stories of preparedness and unpreparedness equally. Participants used their smartphones to audio-record their LADs and return them via email. We corresponded with participants weekly, sending LAD reminders, acknowledging each LAD returned, and asking follow-up questions. In total, we received 136 LADs, which lasted on average 8 min (range 2–22), amounting to 17 h and 10 min of data. LAD participation lasted on average 10 weeks (range 2–14), with participants submitting on average 7 LADs (range 2–12). See Online Supplementary Table for LAD participant details. LAD participants were invited to complete the third phase.
In the third phase, exit interviews, we spoke to 15 participants (79%) in six group interviews (4 medicine groups, 2 pharmacy groups) and one individual interview (medicine) (Mar–Apr 2020). We conducted the interviews in-person or via Zoom, depending on participants’ availability and preferences. We modelled our discussion guide on that used in the entrance interviews, with added emphasis on what had changed through time and why (i.e., their ‘long story’: see Appendix 1 ). Exit interviews lasted on average 69 min (range 53–86), generating 8 h and 3 min of data.
Data analysis
We analysed our QLR data cross-sectionally (RQ1) and longitudinally (RQ2), as well as comparatively (both RQs) following the five-stage framework method (Ritchie & Spencer, 1994 ).
Stage 1, familiarisation : Each team member independently reviewed two of 10 transcripts by listening to the relevant audio-recording while reading each transcript. We annotated the transcripts with our thoughts relating to the research questions, summarising our key points at the end of each transcript.
Stage 2, identifying the thematic framework : All team members met to discuss key points, pulling these together into a preliminary coding framework. This was further developed, including contextual themes (e.g., narrative type, such as prepared story) and conceptual themes (e.g., narrative focus, such as communication), along with definitions and examples for each theme. Development of the coding framework was inductive and deductive, drawing on published research (Monrouxe et al., 2014 , 2018 ), national competency standards (e.g., Pharamaceutical Society of Australia, 2016 ) and intern outcome statements (e.g., Australian Medical Council & Medical Board of Australia, 2013 ).
Stage 3, indexing : Two team members (CK, EO) used the coding framework to code transcripts in NVivo (Version 12.2.0, QSR International). We first located narratives in participants’ talk, then coded the narrative type: prepared story, unprepared story, both (i.e., story with prepared and unprepared elements), or unclear. Next, we coded the narrative focus, using higher order and sub-themes. Sometimes narratives were coded to multiple foci. CK and EO met regularly to discuss coding progress and any challenges encountered, revising the coding framework as required.
Stage 4, charting : We used matrix coding queries to explicate data patterns, such as dominant narrative types over and through time, and similarities and differences in narrative foci between medicine and pharmacy graduates. In this way, we identified and explored preparedness longitudinally (e.g., through time at the individual level, and over time at discipline and cohort levels) and cross-sectionally (e.g., by discipline). So, we viewed/treated time as both fluid and fixed (Balmer & Richards, 2022 ; Balmer et al., 2021 ). While we explored patterns through “credentialing counting” (i.e., frequencies and percentages helping us evidence our interpretations: Monrouxe & Rees, 2020 , p. 186), we ‘closet’ (i.e., hide) frequencies and percentages when presenting our findings to avoid undermining our nuanced/complex qualitative meaning-making, which is possible if readers privileged quantities rather than qualities (Hannah & Lautsch, 2011 ; Monrouxe & Rees, 2020 ). Furthermore, we developed two pen portraits (reports for individual cases that: “successfully concentrate a large amount of longitudinal qualitative data into a focused account”: Sheard & Marsh, 2019 , p. 2–3) to better understand and illustrate the longitudinal narratives from one medical intern and one pharmacy intern, chronologically documenting their transition journeys, and highlighting developments through time (Neale, 2018 ; Sheard & Marsh, 2019 ). Note that we selected these two participants because they were involved in all three study phases, and with rich data to illustrate their diverse experiences.
Stage 5, mapping and interpretation : We interpreted our findings firstly by drawing upon published literature relating to preparedness, transitions, and QLR. We secondly interpreted our comparative findings to make sense of their implications for multiprofessional learning opportunities.
Research team and reflexivity
All eight members of our authorship team for this paper have health/education-related backgrounds (3 dietetics, 2 pharmacy, 2 psychology, 1 medicine). Six have clinical experience, five are experienced educators, and three held teaching/coordinating roles in the degrees sampled during the study. The three team members responsible for participant recruitment and data collection (CK, KML, EO) had no prior relationships with participants. Undertaking a team reflexivity activity at the start of our research (to discuss our backgrounds, expertise, philosophical positioning, hopes and fears for the project) supported an understanding and appreciation of the clinical and educational diversity within our team, strengthening our ability to interpret and contextualise the findings (Barry et al., 1999 ).
We identified 424 narratives in participants’ data. Of these, 222 were coded as unprepared, and 160 as prepared. A further 37 contained both prepared and unprepared elements, and 5 were unclear. For clarity, in this paper we focus only on the 382 narratives that were coded as prepared or unprepared (except in the longitudinal pen portraits, where we synthesise and report data from two participants, irrespective of narrative type).
RQ1: What are the key areas of perceived preparedness and unpreparedness for medicine and pharmacy graduates, and how do they compare between the professions?
Across the 382 narratives, participants’ stories sometimes focused on multiple higher order themes, which were: practical skills and tasks, interpersonal skills, knowledge, and professional practice. Despite guidance to share prepared and unprepared stories equally, of the 229 stories recounted by medicine participants, there were substantially more unprepared stories than prepared stories. However, of the 153 stories narrated by pharmacy participants, there were similar numbers of unprepared and prepared stories. A synthesis of our RQ1 findings across the four higher order themes is visually represented in Fig. 2 .

Visual representation of our RQ1 findings across the four higher order themes. This figure illustrates the four higher order themes (i.e., practical skills and tasks, interpersonal skills, knowledge, and professional practice) in medicine and pharmacy participants’ preparedness narratives. The thumbs up and thumbs down icons reflect the dominant sub-themes for which participants reported feeling prepared and unprepared for, respectively
Feelings of preparedness for practical skills and tasks
Participants narrated more unprepared stories about practical skills and tasks than prepared stories. Unprepared stories were primarily about patient management, such as difficulties with medications, discharge summaries, suboptimal handover, patients with multiple comorbidities, and management plans. Emergency situations, including Medical Emergency Team calls, and deteriorating or aggressive patients were also challenging for new graduates. Unprepared time management stories included struggling with busy/fast-paced environments, triaging/prioritising tasks, working overtime, and efficiency. This is illustrated by a female pharmacy graduate, who describes her unpreparedness for efficiently completing medication reconciliations in one of her LADs:
“… I had to do the med recs [medication reconciliations]… when you haven’t been on a ward before… when you go through the patient notes, a lot of it is medical abbreviation and jargon… and so it takes me a little while to research it, and then put it into context. And then going through notes after notes. It’s a very time-consuming process…” (FG17P3P1F).
Prepared stories commonly focused on patient management, such as comfort with reviewing patients, medications/fluids, discharge summaries, management plans, writing referrals, and completing tasks/procedures. For example, a female medicine graduate describes her preparedness for catheterising a patient in one of her LADs:
“… this co-intern… they left… before they got a chance to do it [catheterise a patient with urinary retention]. So, I ended up putting the catheter in… I could do this procedure without needing any supervision, without needing to ask for anything. And it went well.” (FG18M5P2F).
Prepared stories about patient assessment included ease with history-taking, performing physical examinations, developing diagnoses and management plans, and reporting back to seniors. Prepared stories were also about medication/IV safety, such as evaluating medication appropriateness, identifying drug interactions and errors, as well as advising on optimal medication timing/duration. Interestingly, medical graduates narrated proportionately more unprepared stories about practical skills and tasks than pharmacy graduates.
Feelings of preparedness for interpersonal skills
Participants recounted more prepared stories about interpersonal skills than unprepared stories. Prepared stories were typically about communication, including comfort with intra/interprofessional interactions (e.g., contacting prescribers, making referrals), completing written documentation (e.g., progress notes, medication charts, discharge summaries), and interviewing/counselling patients and family members. Prepared autonomy stories also included doing activities independently (e.g., making decisions, solving problems). Prepared stories about teamwork/collaboration included ease with building relationships, supporting new team members, requesting/accepting support, and assisting colleagues. For example, one female medicine graduate explains in her entrance interview how she felt prepared to contribute to the workload of the medical team in one of her final year rotations:
“I had a rotation in gen med… There’d be so much paperwork… me and [fellow medical student] had to step up and kind of, help out with the workload of the team, else we would never finish... having the chance to actually do stuff, was actually probably the most important thing [for helping feelings of preparedness]…” (FG11M2P2F).
Unprepared stories predominately focused on communication, including challenges with interviewing/counselling patients and family members (e.g., non-English speakers, breaking bad news, emotional individuals, conflict management), completing written documentation, interacting with seniors (e.g., case presentations, responding to criticism), and intra/interprofessional interactions. Unprepared stories about teamwork/collaboration included difficulties getting along with others, negotiating hierarchies, managing differing opinions, task delegation, and advice/information seeking. For example, one female pharmacy graduate describes in her exit interview her unpreparedness for challenging a medical prescriber’s prescription:
“I took the script down to the pharmacy, and I started dispensing it, and I was kind of like, ‘hmm, this doesn’t seem right’… I said to the pharmacist in the dispensary… ‘Oh, they’ve done this, but they actually need to do this.’ And they’re like, ‘Well, in that case, you need to contact the prescriber.’ I was like, ‘Oh, no, I don’t want to do that.’ [laughs]. And they were like, ‘Well, you’ve got to’…” (FG15P1P1F).
Unprepared accountability/responsibility stories included struggling with running clinics, writing/dictating letters, answering patients’/colleagues’ questions, and escalating care. Interestingly, pharmacy graduates narrated proportionately more prepared and unprepared stories about interpersonal skills than medical graduates.
Feelings of preparedness for knowledge
There were slightly more unprepared stories narrated about knowledge than prepared stories. Unprepared stories primarily focused on clinical knowledge, including challenges with pharmacy internship exam preparation, feeling pressured to have the right answer, encountering unfamiliar scenarios, and lacking knowledge about tests, treatments, and devices. Unprepared knowledge application stories included mind blanks when treating/counselling patients and realising the need to practise skills/tasks and build experience. A female pharmacy graduate describes her unpreparedness in one of her LADs regarding her knowledge of a specific antidepressant:
“[My preceptor] quizzed me on an antidepressant… It was a simple antidepressant… and I thought I knew it. Clearly, I didn’t know as well as I should have. So, I’ve still got a long way to go.” (FG16P2P1F).
Prepared stories were commonly about clinical knowledge, such as comfort with learning/retaining content about conditions, procedures, and medications, answering questions, knowing when to ask for help, and locating information. A female medicine graduate explains in one of her LADs her preparedness for finding information:
“The other thing that I think I’ve been prepared for well is when I don’t know what to do, I can look it up very easily. And we’ve been given a whole bunch of resources that we’ve used throughout med school… that’s been really good to know exactly where to go and how to look something up.” (FG10M1P2F).
Prepared stories about knowledge application included ease with drawing on different information to develop/initiate management plans, identifying medication errors and suggesting alternatives, and recalling information to provide advice. Intriguingly, pharmacy graduates narrated proportionately more unprepared stories about knowledge than medical graduates.
Feelings of preparedness for professional practice
There were slightly more unprepared stories recounted about professional practice than prepared stories. Unprepared stories were predominately about participants’ own health/wellbeing, including difficulties adjusting to full-time work as interns (e.g., night shifts and weekends), establishing routines, maintaining work/life/study balance, taking breaks and personal leave, and managing emotions, exhaustion, and stress. Unprepared lifelong learning stories included challenges with identifying learning goals, keeping abreast of industry news, and exam preparation. Unprepared stories were also about scope of practice, including understanding local prescribing protocols and when to refer to other disciplines. This is illustrated by a male medicine graduate in his exit interview:
“I guess scope of practice is something that I’m still trying to determine… when it’s a good idea to page or request an assessment from other professionals… when a consultant especially asks a task to be done by you, I find it a bit difficult to say, ‘Is it alright if I hand it over to someone else?’...” (FG11M2P1M).
Prepared stories typically focused on lifelong learning, such as comfort with internship training, exam preparation, accepting/learning from mistakes, accessing resources, and drawing on others’ expertise to develop knowledge/skills. Prepared stories about participants’ own health/wellbeing included ease with establishing routines, undertaking self-care activities, and maintaining work/life balance. Prepared self-evaluation stories included mid/end of rotation assessments, participants evaluating their own emotional states and impacts, and critically reflecting on their practice. This is illustrated by a female pharmacy graduate in one of her LADs:
“And other aspects that I enjoyed this week was when I was with more organised pharmacists in the dispensary, and they gave me the opportunity to counsel patients… when I finish counselling, I can reflect back on myself, my performance, and see areas that I could improve on… then when I speak to the next patient, I just try and incorporate the things that I thought I was missing...” (FG16P2P2F).
Interestingly, medical graduates narrated proportionately more unprepared stories about professional practice than pharmacy graduates.
Across the 382 narratives, participants reported substantially fewer narratives before starting internship, compared to during internship. Before internship, narratives were about interpersonal skills, knowledge, practical skills and tasks, and professional practice. Narratives reported during internship commonly focused on practical skills and tasks, interpersonal skills, knowledge, and professional practice. While medicine participants recounted roughly equal numbers of unprepared and prepared stories before internship, there were substantially more unprepared stories during internship. They narrated more prepared stories about interpersonal skills and professional practice before internship, but more unprepared stories for these two themes during internship. They narrated equal numbers of prepared and unprepared stories about knowledge before internship, but this shifted to more unprepared stories during internship. They narrated more unprepared stories about practical skills and tasks before and during internship. Interestingly, pharmacy participants recounted roughly equal numbers of unprepared and prepared stories before and during internship. They narrated more prepared stories about practical skills and tasks, and professional practice before internship. While this positive trend continued during internship for professional practice, the dominant narrative type for practical skills and tasks changed to unprepared. They narrated equal numbers of prepared and unprepared stories about interpersonal skills before internship, but this shifted to more prepared stories during internship. Also showing a positive trend was preparedness for knowledge, where the dominant narrative type changed from unprepared before internship, to prepared during internship. A synthesis of our RQ2 cohort findings over time is visually represented in Fig. 3 .

Visual representation of our RQ2 cohort findings over time. This figure illustrates the dominant narrative types (i.e., prepared = thumbs up or unprepared = thumbs down) for each of the four higher order themes, by profession and time-period. Note that ‘Before internship’ reflects data collected in Phase 1, while ‘During internship’ encompasses data collected in Phases 2 and 3
Changes over time: cohort patterns
In terms of practical skills and tasks, participants consistently recounted more unprepared stories over time. Although unprepared stories before internship commonly focused on patient assessment, patient management, and time management, during internship, they were often about patient management, time management, and emergency situations. Prepared stories before internship were about patient management and patient assessment, yet during internship, they centred on patient management, medication/IV safety, patient assessment, and workplace systems like comfort with electronic medical records, incident reporting, and human resources. Only medical students narrated unprepared stories about practical skills and tasks before internship. Furthermore, medical graduates narrated proportionately more unprepared stories about practical skills and tasks during internship than pharmacy graduates. Pharmacy graduates’ unprepared stories about practical skills and tasks increased over time. Regarding interpersonal skills, participants consistently narrated more prepared stories over time. Prepared stories before internship predominately focused on communication, teamwork/collaboration, and accountability/responsibility. During internship, preparedness for communication and teamwork/collaboration remained common, with the addition of autonomy. While unprepared stories before internship were mostly about communication, accountability/ responsibility, and therapeutic relationships, during internship, they focused on communication, teamwork/collaboration, and accountability/responsibility. Before internship, medical students narrated proportionately fewer unprepared stories about interpersonal skills than pharmacy students. While this pattern continued during internship, the difference was less marked. Concerning knowledge, participants consistently reported more unprepared stories over time. Unprepared stories before and during internship were primarily about clinical knowledge and knowledge application. Similarly, prepared stories before and during internship were typically about clinical knowledge and knowledge application. Before internship, medical students narrated proportionately fewer unprepared stories about knowledge than pharmacy students. While this pattern continued during internship, the difference was less marked. Finally, relating to professional practice, participants narrated more prepared stories before internship, but more unprepared stories during internship. While prepared stories before internship were about participants’ own health/wellbeing, lifelong learning, and scope of practice, during internship, they centred on self-evaluation, lifelong learning, and participants’ own health/wellbeing. Although unprepared stories before internship were about participants’ own health/wellbeing, and lifelong learning, during internship, they focused on participants’ own health/wellbeing, scope of practice, safe practice, and lifelong learning. Only medical students narrated unprepared stories about professional practice before internship. Furthermore, medical graduates narrated proportionately more unprepared stories about professional practice during internship than pharmacy graduates. Pharmacy graduates’ unprepared stories about professional practice increased over time.
Changes through time: illustrative pen portraits
Pen portraits are now presented to illustrate two longitudinal cases (one medicine, one pharmacy). The first case is that of Josie (pseudonym), a female medical graduate (Box 1 ). She participated in an entrance interview, 10 LADs through an 11-week period, and an exit interview, providing 3 h and 58 min of data (weeks 0–23). As a final year student, Josie talked about her placements in rural and metropolitan health services, including in an emergency department. Upon graduation, she began her internship with a 10-week general surgical rotation in a metropolitan health service, before moving to a general medical rotation at a different hospital within the same health service. Josie’s exit interview took place approximately three weeks into her second rotation. The second case is that of Hannah (pseudonym), a female pharmacy graduate (Box 2 ). She participated in an entrance interview, 12 LADs through an 11-week period, and an exit interview, culminating in 4 h and 44 min of data (weeks 0–19). As a final year student, Hannah talked about her placements in community and hospital settings, including on general medicine and renal wards. Upon graduation, she started her internship with a 5-week rotation on a general medical ward in a regional health service. She then moved to the hospital dispensary for a short time, before rotating to a surgical ward with the same health service. Hannah’s exit interview took place approximately four weeks into her time on the surgical ward.
This comparative study explores medical and pharmacy learners’ perceptions of preparedness and unpreparedness, and how these feelings change over the final year student-new graduate transition. Our comparative analysis also provides insights into opportunities for multiprofessional learning before and during new graduate transitions. In this discussion, we first summarise our key findings and compare these with existing literature and theory, especially illustrating where our study extends existing research. We then outline the methodological strengths and limitations of the study, before concluding with the implications of the findings for further research and educational practice.
Summary of key findings and comparison with existing literature and temporal theory
Regarding RQ1, several findings were consistent with existing literature: (a) participants’ examples of preparedness and unpreparedness involving practical skills and tasks, interpersonal skills, and knowledge (e.g., Monrouxe et al., 2017 ; Padley et al., 2021 ); (b) unprepared stories dominating participants’ narratives involving practical skills and tasks such as patient management, time management, and emergency situations (Brinkman et al., 2018 ; Burridge et al., 2020 ; James & Cole, 2016 ); (c) prepared stories dominating participants’ narratives about interpersonal skills such as communication, teamwork/collaboration, and autonomy (Lefroy et al., 2017 ; Monrouxe et al., 2018 ); (d) us coding slightly more unprepared stories involving knowledge like clinical knowledge and knowledge application (Malau-Aduli et al., 2022 ; Merga, 2016 ; Rutter et al., 2013 ); and (e) us coding slightly more unprepared stories involving professional practice such as own health/wellbeing, scope of practice, and lifelong learning (Baten et al., 2018 ; Lundin et al., 2018 ; Merga, 2016 ; Monti et al., 2020 ).
However, our findings for RQ1 extend this literature in several important ways. Firstly, we found that unprepared stories involving practical skills and tasks were especially dominant in medical graduates’ data. Their preoccupation with practical skills and tasks might reflect a broader scope of practice requiring them to enact (and worry about) a wider range of practical skills and tasks than pharmacy graduates. Secondly, we found that prepared and unprepared stories involving interpersonal skills were particularly dominant in pharmacy graduates’ data, suggesting that they were especially preoccupied with their preparedness for interpersonal skills. This preoccupation may reflect this cohort’s traditional knowledge-focused pharmacy curriculum, with only 60 days of experiential placements, before the pharmacy curriculum’s transformation to become more experiential and skills-based including communication and teamworking (Forrester et al., 2023 ). Thirdly, we found that unprepared stories involving knowledge were especially dominant in pharmacy graduates’ data. Their preoccupation with knowledge may reflect the knowledge-focused instruction and assessment that was dominant in their program at that time. It may also reflect pharmacy graduates’ anxieties about causing harm through medication errors, or inaccurate medicines information provided to patients and doctors. Finally, we found that unprepared stories involving professional practice were especially dominant in medical graduates’ data. Their preoccupation with professional practice might reflect their regular night/weekend working affecting their home life more than pharmacy graduates, as well as their challenges with patient management in terms of breaking bad news and death and dying, affecting their coping.
Regarding RQ2, comparing learner experiences before and during internship and thus conceptualising time as fixed and synchronic (Audulv et al., 2022 ; Balmer & Richards, 2022 ; Balmer et al., 2021 ), we found some cohort/discipline evidence of apparent stability over time, as has been found in existing literature (e.g., Chaou et al., 2021 ; Chow et al., 2022 ; Mak et al., 2013 ). In our study sample, we found that unprepared stories involving practical skills and tasks dominated before and during internship for medical participants, and prepared stories about professional practice dominated before and during internship for pharmacy participants. However, we also found cohort/discipline evidence of changes over time, consistent with existing literature (e.g., Chaou et al., 2021 ; Chow et al., 2022 ; Mak et al., 2013 ). In our study sample, while prepared stories were dominant in medical students’ data before internship, unprepared stories dominated during internship, illustrating that medical graduates were especially preoccupied with their unpreparedness for interpersonal skills, knowledge, and professional practice during internship. Conversely, unprepared stories (e.g., involving knowledge, interpersonal skills) were dominant in pharmacy students’ data before internship, yet prepared stories dominated during internship. Furthermore, while prepared stories dominated in pharmacy students’ narratives about practical skills and tasks before internship, unprepared stories dominated during internship.
However, conceptualising time as fluid and diachronic, we found in our two pen portraits changes through time; with evidence of the complexities and nuances of preparedness shifting through time, consistent with one previous UK study of junior doctors published in grey literature (Monrouxe et al., 2014 ). Bringing novelty to the literature, we identified examples of Josie (the medical graduate) and Hannah (the pharmacy graduate) feeling prepared before internship, but then unprepared during internship (e.g., inserting cannulas for Josie, knowledge for Hannah), examples of improved feelings of preparedness during the first three months of work as interns (e.g., cover shifts for Josie, interpersonal skills with colleagues for Hannah), and examples of persistent feelings of unpreparedness over that same time period (e.g., knowledge for Josie, interpersonal skills with patients for Hannah). Indeed, through the entrance/exit interviews and longitudinal audio-diaries, as well as the presentation of in-depth longitudinal pen portraits, we were able to witness the unfolding of Josie and Hannah’s preparedness journeys as they orientated themselves to past, present and future (prospective-retrospective) over a relatively short but intensive time-period (Audulv et al., 2022 ; Balmer et al., 2021 ; Neale, 2018 , 2019 ). Interestingly, this conceptualisation of time as diachronic, subjective, fluid and dynamic (Audulv et al., 2022 ; Balmer & Richards, 2022 ; Balmer et al., 2021 ; Neale, 2018 , 2019 ), clearly illustrated preparedness journeys as non-linear with “detours” and “reversals” mentioned by Balmer et al. ( 2021 , p. 1254).
Methodological strengths and challenges
We collected over 34 h of audio data with 19 medicine and pharmacy participants. Our sample had adequate information power given our narrow study aim (exploring preparedness during the final year student-new graduate transition), dense sample specificity (purposive sampling of final year students from two professions), application of established theory across our broader research program (Multiple and Multidimensional Transitions theory: Jindal-Snape, 2016 ; Rees et al., in press), high-quality interview dialogue (strong researcher-participant rapport supporting the collection of relevant and rich data), and our in-depth analysis strategy (cross-sectional and longitudinal comparative narrative analyses: Malterud et al., 2016 ). We experienced minimal attrition (four participants did not complete an exit interview), by using various engagement strategies including sending regular LAD reminders, acknowledging LAD receipt, providing reassuring feedback on LADs, returning LAD transcripts to participants, and providing $10 gift cards for each study phase completed. We also conducted a rigorous and reflexive team-based analysis of voluminous qualitative data, employing NVivo, which helped us to make sense of our data (the whole dataset, as well as individual cases) cross-sectionally and longitudinally.
However, our study is not without its challenges, and these must be considered before drawing conclusions. First, although our findings are largely supportive of existing international research, our study was conducted in one Australian university only, so our findings (and study implications) may lack transferability to non-Australian contexts with different models of healthcare education and service delivery. Second, given our funding constraints, we collected data over a relatively modest time-period (6-months); shorter than other longitudinal studies (e.g., Chaou et al., 2021 ; Mak et al., 2013 ; Monrouxe et al., 2014 ), and the time-periods suggested for graduates to feel prepared (e.g., Burridge et al., 2020 ; Walker et al., 2013 ). However, timeframe and tempo are often inter-connected in QLR (Rees & Ottrey, in press), so the relatively short duration is partly compensated for by the intensive weekly tempo of data collection for LADs. Plus, this study fills an important gap in the literature on early transitions into clinical practice in pharmacy (Brennan et al., 2024 ). Furthermore, our participants mostly identified as female and Oceanian, so our findings may not represent the experiences of those identifying as male or from an ethnic minority. Finally, our QLR findings outline patterns of dominance in participants’ narratives, which are not to be confused with prevalence of preparedness or unpreparedness across time. Indeed, despite us asking participants for equal numbers of prepared and unprepared stories across their transitions, we know that emotional experiences are more likely to be remembered and narrated (Rees et al. 2013 ), potentially accounting for the dominance in unprepared narratives across our study. However, this is an important finding in of itself, as we can see clearly in our QLR findings what issues students are most preoccupied with in terms of their preparedness and when, suggesting when they may be most receptive to transition interventions (and on what topics).
Study implications
Given our study challenges, we recommend that further research is conducted at non-Australian universities (representing different models of healthcare education and service delivery) to establish the transferability of our findings to wider-ranging contexts. We also encourage researchers to conduct QLR across longer study durations to track the ebbs and flows of preparedness for practice across the internship year, and into full registration. Finally, further research should encourage the participation of students and graduates representing demographics underrepresented in this study (e.g., those identifying as male, and culturally and linguistically diverse professionals).
Regarding educational implications, this study set out to understand what (if any) opportunities exist to develop multiprofessional transition to practice interventions, when these interventions should be optimally timed, and on what topics. In Table 2 , we outline recommendations for educators based on our findings. While the cross-sectional findings for RQ1 imply that uniprofessional transition interventions could be preferred (because medical and pharmacy learners are preoccupied with unpreparedness for different things), our longitudinal findings for RQ2 clearly indicate opportunities for multiprofessional transition interventions in final year and during the first few months of work as interns.
Data availability
We do not have ethics approval to share our data openly, in order to protect the privacy of our study participants.
Audulv, Å., Hall, E. O. C., Kneck, Å., Westergren, T., Fegran, L., Pedersen, M. K., Aagaard, H., Dam, K. L., & Ludvigsen, M. S. (2022). Qualitative longitudinal research in health research: A method study. BMC Medical Research Methodology, 22 , 255.
Article Google Scholar
Australian Medical Council & Medical Board of Australia, (2013) Intern training—intern outcome statements. Australian Medical Council. Canberra, Australia. Available from: https://www.amc.org.au/images/intern-training/intern-training-intern-outcome-statements-2014-09-24.pdf (Accessed 15 June 2023)
Balmer, D. F., & Richards, B. F. (2022). Conducting qualitative research through time: How might theory be useful in longitudinal qualitative research? Advances in Health Sciences Education, 27 , 277–288.
Balmer, D. F., Varpio, L., Bennett, D., & Teunissen, P. W. (2021). Longitudinal qualitative research in medical education: Time to conceptualise time. Medical Education, 55 , 1253–1260.
Barry, C. A., Britten, N., Barber, N., Bradley, C., & Stevenson, F. (1999). Using reflexivity to optimize teamwork in qualitative research. Qualitative Health Research, 9 , 26–44.
Baten, A., Bleeker-Rovers, C. P., van den Heijkant, F., de Graaf, J., & Fluit, C. R. M. G. (2018). Residents’ readiness for out-of-hours service: A Dutch national survey. Netherlands Journal of Medicine, 76 (2), 78–83.
Google Scholar
Blair, M., Mitchell, L., Gibson, S., Rees, C. E., Ottrey, E., Monrouxe, L. V., & Palermo, C. (2023). The graduate dietitian experience of employment and employability: A longitudinal qualitative research study from one Australian university. Nutrition and Dietetics, 80 , 377–388.
Brennan, N., Burns, L., Mattick, K., Mitchell, A., Henderson, T., Walker, K., & Gale, T. (2024). How prepared are newly qualified allied health professionals for practice in the UK? A Systematic Review. BMJ Open, 14 , e081518.
Brinkman, D. J., Tichelaar, J., Graff, S., Otten, R. H. J., Richir, M. C., & van Agtmael, M. A. (2018). Do final-year medical students have sufficient prescribing competencies? A systematic literature review. British Journal of Clinical Pharmacology, 84 , 615–635.
Burr, V. (2015). Social constructionism . Routledge.
Book Google Scholar
Burridge, S., Shanmugalingam, T., Nawrozzadeh, F., Leedham-Green, K., & Sharif, A. (2020). A qualitative analysis of junior doctors’ journeys to preparedness in acute care. BMC Medical Education, 20 , 12.
Cameron, A., Millar, J., Szmidt, N., Hanlon, K., & Cleland, J. (2014). Can new doctors be prepared for practice? A review. The Clinical Teacher, 11 , 188–192.
Chanakit, T., Low, B. Y., Wongpoowarak, P., Moolasarn, S., & Anderson, C. (2015). Hospital pharmacists’ perceptions of the suitability of doctor of pharmacy graduates in hospital settings in Thailand. BMC Medical Education, 15 , 181.
Chaou, C.-H., Yu, S.-R., Chang, Y.-C., Ma, S.-D., Tseng, H.-M., Hsieh, M.-J., & Fang, J.-T. (2021). The evolution of medical students’ preparedness for clinical practice during the transition of graduation: A longitudinal study from the undergraduate to postgraduate periods. BMC Medical Education, 21 , 260.
Chow, A., Chen, S., Rosby, L., Low-Beer, N., Shelat, V. G., Cleland, J., Cartlam, B., & Smith, H. E. (2022). Student assistantship programme: An evaluation of impact on readiness to transit from medical student to junior doctor. BMC Medical Education, 22 , 99.
Corfield, L., Williams, R. A., Lavelle, C., Latcham, N., Talash, K., & Machin, L. (2021). Prepared for practice? UK Foundation doctors’ confidence in dealing with ethical issues in the workplace. Journal of Medical Ethics, 47 , e25.
Ebert, L., Hoffman, K., Levett-Jones, T., & Gilligan, C. (2014). “They have no idea of what we do or what we know”: Australian graduates’ perceptions of working in a health care team. Nurse Education in Practice, 14 , 544–550.
Forrester, C. A., Lee, D. S., Hon, E., Lim, K. Y., Brock, T. P., Malone, D. T., Furletti, S. G., & Lyons, K. M. (2023). Preceptor perceptions of pharmacy student performance before and after a curriculum transformation. American Journal of Pharmaceutical Education, 87 (2), ajpe8575.
Gordon, L., Jindal-Snape, D., Morrison, J., Muldoon, J., Needham, G., Siebert, S., & Rees, C. (2017). Multiple and multidimensional transitions from trainee to trained doctor: a qualitative longitudinal study in the UK. British Medical Journal Open . https://doi.org/10.1136/bmjopen-2017-018583
Gordon, L., Rees, C. E., & Jindal-Snape, D. (2020). Doctors’ identity transitions: Choosing to occupy a state of ‘betwixt and between.’ Medical Education, 54 , 1006–1018.
Hannah, D. R., & Lautsch, B. A. (2011). Counting in qualitative research: Why to conduct it, when to avoid it, and when to closet it. Journal of Management Inquiry, 20 (1), 14–22.
Hawkins, N., Younan, H.-C., Fyfe, M., Parekh, R., & McKeown, A. (2021). Exploring why medical students still feel underprepared for clinical practice: A qualitative analysis of an authentic on-call simulation. BMC Medical Education, 21 , 165.
James, P. B., & Cole, C. P. (2016). Intern pharmacists’ perceived preparedness for practice, their extent of involvement in pharmacy related activities and future career choices in Sierra Leone: A baseline descriptive survey. Pharmacy Education, 16 , 26–32.
Jee, S. D., Schafheutle, E. I., & Noyce, P. R. (2017). Using longitudinal mixed methods to study the development of professional behaviours during pharmacy work-based training. Health and Social Care in the Community, 25 , 975–986.
Jindal-Snape, D. (2016). A-Z of Transitions . Palgrave.
Kitto, S. C., Chesters, J., & Grbich, C. (2008). Quality in qualitative research. Medical Journal of Australia, 188 , 243–246.
Lefroy, J., Yardley, S., Kinston, R., Gay, S., McBain, S., & McKinley, R. (2017). Qualitative research using realist evaluation to explain preparednbess for doctors’ memorable ‘firsts.’ Medical Education, 51 , 1037–1048.
Lundin, R. M., Bashir, K., Bullock, A., Kostov, C. E., Mattick, K. L., & Monrouxe, L. V. (2018). “I’d been like freaking out the whole night”: Exploring emotion regulation based on junior doctors’ narratives. Advances in Health Sciences Education, 23 , 7–28.
Magola, E., Willis, S. C., & Schafheutle, E. I. (2018). Community phamacists at transition to indepent practice: Isolated, unsupported, and stressed. Health and Social Care in the Community, 26 , 849–859.
Mak, V. S. L., March, G., Clark, A., & Gilbert, A. L. (2013). Australian intern pharmacists’ perceived preparedness for practice, and their expectations and experiences of the internship year and future career intentions. Integrated Pharmacy Research and Practice, 2 , 25–34.
Malau-Aduli, B. S., Jones, K., Alele, F., Adu, M. D., Dronvandi, A., Knott, G., Young, L., & Jo, C. (2022). Readiness to enter the workforce: Preceptions of health professions students at a regional Australian university. BMC Medical Education, 22 , 89.
Malterud, K., Siersma, V. D., & Guassora, A. D. (2016). Sample size in qualitative interview studies: Guided by information power. Qualitative Health Research, 26 , 1753–1760.
Merga, M. (2016). Gaps in work readiness of graduate health professional and impact on early practice: Possibilities for future interprofessional learning. Focus on Health Professional Education: A Multi-Disciplinary Journal, 17 (3), 14–29.
Michaelides, A., Mahr, M., Pydisetty, G., & Loyala, J. V. (2020). Assessing the preparedness of foundation year 1 (FY1) doctors during the tansition from medical school to the foundation training programme. BMC Medical Education, 20 , 106.
Monrouxe, L., Bullock, A., Cole, J., Gormley, G., Kaufhold, K., Kelly, N., Mattick, K., Rees, C., & Scheffler, G. (2014) How prepared are UK medical graduates for practice? Final report from a programme of research commissioned by the General Medical Council. London: General Medical Council. Available from: https://www.gmc-uk.org/-/media/gmc-site/about/how-prepared-are-uk-medical-graduates-for-practice.pdf (Accessed 15 June 2024)
Monrouxe, L. V. (2009). Solicited audio diaries in longitudinal narrative research: A view from inside. Qualitative Research, 9 , 81–103.
Monrouxe, L. V., Bullock, A., Gormley, G., Kaufhold, K., Kelly, N., Robert, C. E., Mattick, K., & Rees, C. (2018). New graduate doctors’ preparedness for practice: A multistakeholder, multicentre narrative study. British Medical Journal Open, 8 , e023146.
Monrouxe, L. V., Grundy, L., Mann, M., John, Z., Panagoulas, E., Bullock, A., & Mattick, K. (2017). How prepared are UK medical graduates for practice? A rapid review of the literature 2009–2014. British Medical Journal Open, 7 , e013656.
Monrouxe, L. V., & Rees, C. E. (2020). When I say… quantification in qualitative research. Medical Eduucation, 54 , 186–187.
Monti, M., Brunet, L., & Michaud, P. A. (2020). Transition to postgraduate practice: Perceptions of preparedness and experience of the daily work of junior residents. Swiss Medical Weekly, 150 , w20370.
Neale, B. (2018). What is qualitative longitudinal research? Bloomsbury Academic.
Neale, B. (2019). Qualitative longitudinal research. In P. Atkinson, S. Delamont, A. Cernat, J. W. Skshaug, & R. A. Williams (Eds.), Sage Research Methods Foundation (pp. 1–15). SAGE.
Neale, B., & Flowerdew, J. (2003). Time, texture and childhood: The contours of longitudinal qualitative research. International Journal of Social Research Methodology, 6 , 189–199.
Ottrey, E., Rees, C. E., Kemp, C., Brock, T. P., Leech, M., Lyons, K., Monrouxe, L. V., Morphet, J., & Palermo, C. (2021). Exploring healthcare graduates’ conceptualisations of preparedness for practice: A longitudinal qualitative research study. Medical Education, 55 , 1078–1090.
Padley, J., Boyd, S., Jones, A., & Walters, L. (2021). Transitioning from university to postgraduate medical training: A narrative review of work readiness of medical graduates. Health Science Reports, 4 , e270.
Parmar, H., Schafheutle, E., Willis, S., & Silkstone, V. (2020). Does curriculum reform influence perceived preparedness for practice of graduates? A comparison of two cohorts. International Journal of Pharmacy Practice, 28 , 156–164.
Pharmaceutical Society of Australia (2016) National competency standards framework for pharmacists in Australia. Deakin West, ACT, Australia. Available from: https://www.psa.org.au/wp-content/uploads/2018/06/National-Competency-Standards-Framework-for-Pharmacists-in-Australia-2016-PDF-2mb.pdf (Accessed 15 June 2024)
Rees, C. E., & Ottrey, E. (in press) “Lives and times”: The case for qualitative longitudinal research in anatomical sciences education. Anatomical Sciences Education . https://doi.org/10.1002/ase.2514 .
Rees, C. E., Crampton, P. E. S., & Monrouxe, L. V. (2020). Re-visioning academic medicine through a constructionist lens. Academic Medicine, 95 , 846–850.
Rees, C., Ottrey, E., Kemp, C., Brock, T., Leech, M., Lyons, K., Monrouxe, L., Morphet, J., & Palermo, C. (2022). Understanding health care graduates’ conceptualizations of transitions: A longitudinal qualitative research study. Academic Medicine, 97 (7), 1049–1056.
Rees, C. E., Ottrey, E., Kemp, C., & Palermo, C. (in press) Chapter 14. Multiple interacting and impacting transitions for new health professional graduates: Extending transitions theory in health professions education. In: Jindal-Snape D, (ed.), The palgrave handbook of multiple and multi-dimensional educational and life transitions . Palgrave Macmillan: London, pp. X–X
Rees, C. E., Monrouxe, L. V., & McDonald, L. A. (2013) Narrative, emotion and action: analysing 'most memorable' professionalism dilemmas. Medical Education , 47 , 80–96.
Riessman, C. K. (2008). Narrative methods for the human sciences . Sage Publications.
Ritchie, J., & Spencer, L. (1994). Qualitative data analysis for applied policy research. In A. Bryman & R. G. Burgess (Eds.), Analyzing Qualitative Data (pp. 173–194). Routledge.
Chapter Google Scholar
Rutter, P., Taylor, D., & Branford, D. (2013). Mental health curricula at schools of pharmacy in the United Kingdom and recent graduates’ readiness to practice. American Journal of Pharmaceutical Education, 77 , 1–7.
Sheard, L., & Marsh, C. (2019). How to analyse longitudinal data from multiple sources in qualitative health research: The pen portrait analytic technique. BMC Medical Research Methodology, 19 , 169.
SmithBattle, L., Lorenz, R., Reangsing, C., Palmer, J. L., & Pitroff, G. (2018). A methodological review of qualitative longitudinal research in nursing. Nursing Inquiry, 25 , e12248.
Sumpradit, N., Suttajit, S., Hunnangkul, S., Wisaijohn, T., & Putthasri, W. (2014). Comparison of self-reported professional competency across pharmacy education programs: A survey of Thai pharmacy graduates enrolled in the public service program. Advances in Medical Education and Practice, 5 , 347–357.
Vogl, S., Zartler, U., Schmidt, E.-M., & Rieder, I. (2018). Developing an analytical framework for multiple perspective, qualitative longitudinal interviews (MPQLI). International Journal of Social Research Methodology, 21 , 177–190.
Waite, N. M., McCarthy, L., Milne, E., Hillier, C., Houle, S. K. D., & Dolovich, L. (2018). Perceived preparedness for full-scope pharmacist services among recent Doctor of Pharmacy graduates from Ontario schools of pharmacy. Journal of the American Pharmacists Association, 58 , 630–637.
Walker, A., Yong, M., Pang, L., Fullarton, C., Costa, B., & Dunning, A. M. T. (2013). Work readiness of graduate health professionals. Nurse Education Today, 33 , 116–122.
Download references
Acknowledgements
We would like to thank all participants for sharing their views and experiences of preparedness with us over their graduate transition. We would also like to thank Julia Harrison and Suzanne Caliph for their assistance with participant recruitment. And we would like to thank other members of the broader research team not co-authoring this paper (Julia Morphet, Monash Nursing & Midwifery).
Open Access funding enabled and organized by CAUL and its Member Institutions. This study was funded by a Monash University Faculty of Medicine, Nursing and Health Sciences 2019 Teaching & Learning Research Grant.
Author information
Authors and affiliations.
Monash Centre for Scholarship in Health Education (MCSHE), Faculty of Medicine, Nursing & Health Sciences, Monash University, Clayton, VIC, Australia
Ella Ottrey, Charlotte E. Rees, Caitlin Kemp & Claire Palermo
School of Health Sciences, College of Health, Medicine & Wellbeing, The University of Newcastle, Callaghan, NSW, Australia
Charlotte E. Rees
Faculty of Pharmacy and Pharmaceutical Sciences, Monash University, Parkville, VIC, Australia
Kayley M. Lyons & Tina P. Brock
Centre for Digital Transformation of Health, Faculty of Medicine, Dentistry and Health Science, University of Melbourne, Melbourne, VIC, Australia
Kayley M. Lyons
Centre for Collaborative Practice, University of Melbourne, Melbourne, VIC, Australia
Tina P. Brock
Medicine Course, Faculty of Medicine, Nursing & Health Sciences, Monash University, Clayton, VIC, Australia
Michelle Leech
School of Health Sciences, Faculty of Medicine and Health, The University of Sydney, Camperdown, Sydney, NSW, Australia
Lynn V. Monrouxe
You can also search for this author in PubMed Google Scholar
Contributions
CER, TPB, ML, LVM, and CP designed and secured funding for the study. EO and CK secured ethics approval. CK, KML and EO were involved in recruitment and collecting data. All authors were involved in analysing and interpreting data. EO and CER wrote the paper, so are joint first authors. All remaining authors commented on and/or edited the paper. All authors give their final approval for this version to be published.
Corresponding author
Correspondence to Charlotte E. Rees .
Ethics declarations
Conflict of interest.
The authors declare no competing interests.
Ethical approval
We received ethics approval from the Monash University Human Research Ethics Committee (Project ID 20026).
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
EO and CER are joint first authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary file1 (DOCX 16 kb)
Appendix 1 illustrations of interview questions and audio-diary prompts*, appendix 1 illustrations of interview questions and audio-diary prompts *.
Entrance interview | LAD prompts | Exit interviews |
|---|---|---|
Can you share with me any memorable experiences from this year where you felt prepared for practice. Can you tell me a story in as much detail as possible? Prompts: What happened, in as much detail as you can remember? Where, when, who was involved, etc. What did you do? What was the reasoning behind what you did? What were you thinking at the time? What did you feel at the time? What helped your preparedness in that scenario? Is there anything that could have helped you to feel even more prepared for practice, and why? Probe: What are the emotional, psychological and social impacts of this memorable experience from your final year, and why? Can you share with me any memorable experiences from this year where you felt unprepared for practice? Prompts: What hindered your preparedness in that scenario? Is there anything that could have helped you to feel more prepared for practice, and why? Probe: | Please share with us an experience from your workplace this week that relates to preparedness/unpreparedness for practice. If you have had multiple experiences this week, please share with us your most memorable positive experience and/or your most memorable negative experience For each audio diary, you might like to use these questions as a guide: Tell us of a time this week when you felt prepared for practice and also a time when you felt less prepared: When and where did the events occur and who else was present? What happened? What did you do? What was the reasoning behind what you did? What were you thinking at the time? What did you feel at the time? How might your preparedness/unpreparedness for practice have influenced this experience and why? If not, why not? Any other comments you want to make about your workplace experiences and preparedness/unpreparedness for practice? | Have you had any other memorable experiences, since your last audio diary, that you haven’t yet shared? Can you share with me any memorable experiences from the past 4 months where you felt prepared for practice? Prompts: What happened, in as much detail as you can remember? Where, when, who was involved, etc. What did you do? What was the reasoning behind what you did? What were you thinking at the time? What did you feel at the time? What helped your preparedness in that scenario? Is there anything from your final year that could have helped you to feel even more prepared for practice, and why? Can you share with me any memorable experiences from the past 4 months where you felt unprepared for practice? Prompts: What hindered your preparedness in that scenario? Is there anything from your final year that could have helped you to feel more prepared for practice, and why? Now I would like to turn your attention to your long story. I hope you have had a chance to skim your audio diaries. Let’s think about preparedness for practice: How have your thoughts about this changed (or not) over time, and why? Prompts: For positive or negative? I noticed initially you felt unprepared for X, later it seemed like you nailed that. How did that feel for you? |
*We only include questions and prompts here relevant to learners’ preparedness for practice experiences focused on in this paper; questions/prompts relevant to conceptualisations of transitions and preparedness, and broader transition experiences are published elsewhere (Ottrey et al., 2021 ; Rees et al., 2022 ; in press). Please contact the corresponding author to request copies of the full discussion and LAD guides.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Ottrey, E., Rees, C.E., Kemp, C. et al. Exploring preparedness transitions in medicine and pharmacy: a qualitative longitudinal study to inform multiprofessional learning opportunities. Adv in Health Sci Educ (2024). https://doi.org/10.1007/s10459-024-10372-w
Download citation
Received : 02 July 2024
Accepted : 08 September 2024
Published : 16 September 2024
DOI : https://doi.org/10.1007/s10459-024-10372-w
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Preparedness
- Transitions
- Qualitative longitudinal research (QLR)
- Longitudinal qualitative research (LQR)
- Find a journal
- Publish with us
- Track your research
DigitalCommons@University of Nebraska - Lincoln
- < Previous Dissertation
Home > gradstudies > UNL Dissertations > 208
Graduate Studies

Dissertations and Doctoral Documents from University of Nebraska-Lincoln, 2023–
Fighting racism and hate: a case study of black graduate students' perceptions of a university president's responses to racialized incidents.
Kaleb L. Briscoe , University of Nebraska-Lincoln Follow
0000-0002-6333-9867
First Advisor
Deryl K. Hatch-Tocaimaza
Committee Members
Christina W. Yao, Stephanie Bondi, Sydney Freeman, Jr., Amanda Morales
Educational Studies (Educational Leadership and Higher Education)
Date of this Version
Document type.
Dissertation
A dissertation presented to the faculty of the Graduate College at the University of nebraska in partial fulfillment of requirements for the degree of Doctor of Philosophy
Major: Educational Studies (Educational Leadership and Higher Education)
Under the supervision of Professor Deryl K. Hatch-Tocaimaza
Lincoln, Nebraska, February 2020
Copyright 2020, Kaleb L. Briscoe.Used by permission
This qualitative, single case study examined Black graduate students’ perceptions of a university president’s responses to racialized incidents and how these perceptions inform Black graduate students’ larger contextual understanding of campus racial climate. Guided by Hurtado et al.’s (2012) Multi-Contextual Model for Diverse Learning Environments, the research questions were: What are Black graduate students’ perceptions of a university president’s responses to racialized incidents at a PWI? How do Black graduate students’ perceptions of a university president’s responses to racialized incidents inform their larger contextual understanding of campus racial climate at a PWI? Data was analyzed on an institutional-level through institutional documents, president statements, and one, 60 minute interview with 4 staff members and on an individual-level through a demographic survey and two, 60-90 minute interviews with 12 Black graduate students from a large, predominantly White institution in the Mid-Atlantic, the University of Maryland.
The findings were displayed through narrative summaries. As a result of the president’s responses to racialized incidents, Black graduate students felt othered, marginalized, and silenced. Findings demonstrated the lack of institutional response strategies that the president of University of Maryland used to address racialized incidents. Overall, participants viewed the president’s responses to racialized incidents as being untimely, inadequate, and inappropriate. Almost all students and staff participants shared that the president’s responses to racialized incidents through campus statements used non-performative and anti-Blackness rhetoric. Black graduate students reported that the president’s responses, from their vantage point, lacked action-oriented language, next steps, and strategies to assist them during the aftermath of the incidents.
The findings from this study underscored a direct connection between the president’s responses to racialized incidents and how Black graduate students at one campus perceive racial climate as being negative. This further illustrates the significance of the role of the presidency when addressing issues of race and racism, and how their responses have the power to disrupt or harm both the personal lived experiences of individuals and the broader campus racial climate for Black graduate students. Several implications for practice and recommendations for theory and future research are offered.
Recommended Citation
Briscoe, Kaleb L., "Fighting Racism and Hate: A Case Study of Black Graduate Students' Perceptions of a University President's Responses to Racialized Incidents" (2020). Dissertations and Doctoral Documents from University of Nebraska-Lincoln, 2023– . 208. https://digitalcommons.unl.edu/dissunl/208
Since September 16, 2024
Included in
Educational Sociology Commons , Higher Education Commons , Inequality and Stratification Commons , Leadership Studies Commons , Race and Ethnicity Commons , Race, Ethnicity and Post-Colonial Studies Commons
Advanced Search
Search Help
- Notify me via email or RSS
- Administrator Resources
- How to Cite Items From This Repository
- Copyright Information
- Collections
- Disciplines
Author Corner
- Guide to Submitting
- gradstudies Website
Home | About | FAQ | My Account | Accessibility Statement
Privacy Copyright
- Open access
- Published: 13 September 2024
Evaluating the implementation of the Pediatric Acute Care Education (PACE) program in northwestern Tanzania: a mixed-methods study guided by normalization process theory
- Joseph R. Mwanga 1 ,
- Adolfine Hokororo 1 , 2 ,
- Hanston Ndosi 1 ,
- Theopista Masenge 2 ,
- Florence S. Kalabamu 2 , 3 ,
- Daniel Tawfik 4 ,
- Rishi P. Mediratta 4 ,
- Boris Rozenfeld 5 ,
- Marc Berg 4 ,
- Zachary H. Smith 6 ,
- Neema Chami 1 , 2 ,
- Namala P. Mkopi 2 , 7 ,
- Castory Mwanga 2 ,
- Enock Diocles 1 ,
- Ambrose Agweyu 8 &
- Peter A. Meaney 4
BMC Health Services Research volume 24 , Article number: 1066 ( 2024 ) Cite this article
Metrics details
In low- and middle-income countries (LMICs), such as Tanzania, the competency of healthcare providers critically influences the quality of pediatric care. To address this issue, we introduced Pediatric Acute Care Education (PACE), an adaptive learning program to enhance provider competency in Tanzania’s guidelines for managing seriously ill children. Adaptive learning is a promising alternative to current in-service education, yet optimal implementation strategies in LMIC settings are unknown.
(1) To evaluate the initial PACE implementation in Mwanza, Tanzania, using the construct of normalization process theory (NPT); (2) To provide insights into its feasibility, acceptability, and scalability potential.
Mixed-methods study involving healthcare providers at three facilities. Quantitative data was collected using the Normalization MeAsure Development (NoMAD) questionnaire, while qualitative data was gathered through in-depth interviews (IDIs) and focus groups discussions (FGDs).
Eighty-two healthcare providers completed the NoMAD survey. Additionally, 24 senior providers participated in IDIs, and 79 junior providers participated in FGDs. Coherence and cognitive participation were high, demonstrating that PACE is well understood and resonates with existing healthcare goals. Providers expressed a willingness to integrate PACE into their practices, distinguishing it from existing educational methods. However, challenges related to resources and infrastructure, particularly those affecting collective action, were noted. Early indicators point toward the potential for long-term sustainability of the PACE, but assessment of reflexive monitoring was limited due to the study’s focus on PACE’s initial implementation.
This study offers vital insights into the feasibility and acceptability of implementing PACE in a Tanzanian context. While PACE aligns well with healthcare objectives, addressing resource and infrastructure challenges as well as conducting a longer-term study to assess reflexive monitoring is crucial for its successful implementation. Furthermore, the study underscores the value of the NPT as a framework for guiding implementation processes, with broader implications for implementation science and pediatric acute care in LMICs.
Peer Review reports
Contributions to the literature
Introduces PACE : This study uniquely evaluated the PACE program in a low-resource setting, offering initial evidence on its implementation and potential impact on pediatric care.
Utilizes the NPT framework : By employing a NPT framework, this research provides a novel methodological example of how to assess the incorporation of e-learning in LMIC clinical settings.
Informs Implementation Strategies : These findings contribute to the design of effective e-learning strategies for healthcare education in LMICs, suggesting practical steps for broader application.
Expands Local Capacity : Demonstrates how PACE can build local healthcare capacity, informing ongoing efforts to sustainably improve pediatric care through education in similar environments.
Context and importance of the study
Pediatric in-service education for healthcare providers in Low- and Middle-income countries (LMICs) often lacks reach, effectiveness, and sustainability, contributing to millions of child deaths annually [ 1 , 2 ]. Pneumonia, birth asphyxia, dehydration, malaria, malnutrition, and anemia cause over 4 million child deaths annually, with half occurring in sub-Saharan Africa and thousands in Tanzania [ 3 , 4 ]. The Tanzanian government aims to reduce neonatal mortality from 20/100,000 to the Sustainable Development Goals (SDGs) target of 12/100,000 by 2030 [ 5 ].
Brief review of the literature
Provider knowledge and skills competency are crucial for care quality in LMICs [ 2 , 6 ]. However, conventional in-service education methods are often inadequate and unsustainable [ 6 ]. These methods do not adapt to individual providers’ knowledge or schedules, target minimal competency, and lack long-term refresher learning, limiting their effectiveness [ 7 , 8 , 9 , 10 ].
Adaptive learning can address these limitations by customizing the timing and sequence of combined e-learning and in-person skills training, creating individualized pathways that reinforce learning and enhance skills competency. This approach helps mitigate manpower and resource shortages in LMICs and represents a strategic innovation in knowledge dissemination.
The World Health Organization (WHO) emphasizes the importance of e-learning solutions for healthcare workers globally [ 11 ]. Adaptive learning, with its capacity to adjust to individual needs, holds significant promise for enhancing training efficiency. However, formal studies on adaptive learning in LMIC contexts are scarce. Establishing best practices in e-learning and adaptive methodologies will enhance the dissemination of evidence-based interventions and improve clinical practice and patient outcomes.
To address current educational limitations for healthcare workers in LMICs, we developed the Pediatric Acute Care Education (PACE) program [ 12 , 13 ]. This adaptive e-learning program offers 340 learning objectives across 10 assignments, covering newborn and pediatric care guidelines for management of seriously ill children. The PACE program’s implementation strategy includes an adaptive e-learning platform optimized for mobile phones, a steering committee, a full-time PACE coordinator, and an escalating nudge strategy to encourage participation.
Study aims and objectives
The primary aim of this research is to assess the preliminary implementation of the PACE intervention across two types of pediatric acute care facilities: zonal hospitals and health centers. The study has two principal objectives: (1) To evaluate the initial PACE implementation in Mwanza, Tanzania, using the constructs of Normalization Process Theory (NPT); (2) To provide insights into its feasibility, acceptability, and scalability potential.
Study design
This study employed a mixed methods approach to evaluate the implementation of the PACE program in three healthcare settings in northwestern Tanzania, nested within a larger pilot implementation of PACE within eight health facilities of the Pediatric Association of Tanzania’s Clinical Learning Network. The study utilized NPT as a framework, combining quantitative and qualitative methods. Quantitatively, a tailored NoMAD survey instrument evaluates the integration of PACE into routine clinical practice. Qualitatively, in-depth interviews and focus group discussions enrich the data.
Theoretical framework
NPT has been described as a sociological toolkit for helping us understand the dynamics of implementing, embedding, and integrating new technology or a complex intervention into routine practice [ 14 ]. NPT provides a conceptual framework for understanding and evaluating the processes (implementation) by which new health technologies and other complex interventions are routinely operationalized in everyday work (embedding) and sustained in practice (integration) [ 15 , 16 , 17 , 18 , 19 , 20 ]. The theory is organized around four main constructs, each of which has its own subconstructs [ 15 ]. These constructs collectively offer insights into the feasibility, acceptability, and scalability of an intervention or innovation (Fig. 1 ). Each of these constructs and subconstructs offers a unique lens through which the feasibility, acceptability, and scalability of a new practice can be evaluated, thereby aiding in its effective implementation.

Boxplot of participant responses to NoMAD survey by NPT construct and subconstruct
Study setting
The study was conducted between August 2022 and July 2023 at three healthcare facilities in Mwanza, Tanzania. The Bugando Medical Centre (BMC), an urban zonal referral and teaching hospital, sees about 7,000 births per year and 6,550 pediatric admissions per year for children aged 1 month to 5 years; the urban Makongoro Health Centre, handles approximately 359 births per year but refers newborn and pediatric admissions to the nearby regional or zonal hospital; and the rural Igoma Health Centre sees about 3,850 births per year and 959 pediatric admissions per year for children aged 1 month to 5 years.
Eligibility criteria
Providers included in the study were required to have a minimum command of English and be actively providing pediatric care to sick patients at least part-time. Eligible providers encompassed a wide range of professional cadres, reflecting the diversity of healthcare providers in Tanzania. These included specialists (medical officers with 3 additional years of specialization), medical officers (5 years of education and 1-year internship), nursing officers (4 years of education and 1-year internship), assistant medical officers (clinical officers with 2 additional years of clinical training), assistant nursing officers (3 years of education), clinical officers (3 years of education), clinical assistants (2 years of education), enrolled nurses (2 years of education), and medical attendants (1 year of education). In addition to providers, senior facility staff with administrative roles who supervise PACE providers, such as ward matrons, medical officers-in-charge, and nursing officers-in-charge, were eligible to participate. The bulk of the care is provided by junior medical officers and nurses, who have limited training and experience caring for children with severe illnesses
Recruitment process
Healthcare providers were informed about the study through their facility leaders, and individuals who responded to the survey were not necessarily the same as those who participated in the focus groups or in-depth interviews.
Data collection tools
Nomad questionnaire.
The NoMAD is a 23-item questionnaire based on the NPT that was designed to assess the social processes influencing the integration of complex interventions [ 18 , 21 ]. It includes 3 general items and 20 related to specific NPT constructs (4 Coherence, 7 Collective Action, 4 Cognitive Participation, 5 Reflexive Monitoring). The general items were scored on a scale of 0-100, and the NPT construct items were modified to include a five-point Likert scale (1-Strongly Agree, 5-Strongly Disagree) and additional options for respondents to indicate whether a question was not relevant to their role, stage, or intervention itself. The NPT subconstruct survey items are listed in Table 1 , and the complete survey is provided in the Supplementary Materials.
In-depth interviews (IDIs) and focus group discussions (FGDs)
Interview guides were developed based on previous experience with similar data collection tools. The training and pretesting of the tools were conducted by the study investigators.
Data collection process
Nomad survey.
All PACE participants were invited via WhatsApp to complete the NoMAD survey directly in REDCap, 30 days post-intervention or upon completion of the PACE course.
Focus group discussions and in-depth interviews
We employed a purposeful sampling strategy for the qualitative components, selecting senior healthcare providers for in-depth interviews (IDIs) and junior providers for focus group discussions (FGDs). This approach ensured junior providers felt comfortable speaking openly, avoiding inhibition from senior participants in focus groups, and facilitated methodological triangulation to enhance the credibility and validity of the findings. Data was triangulated using three different types: methodological triangulation with IDIs and FGDs, investigator triangulation with different research assistants collecting data, and data triangulation using data from IDIs, FGDs and NoMAD surveys. Data collection began with a series of field visits, guided by NPT constructs, and included IDIs and FGDs. FGDs, segregated by sex but including a mix of cadres from each health facility, enriched the diversity of perspectives. The iterative nature of our methodology allowed for continuous refinement of our theoretical framework, methodologies, and sampling strategies, informed by emerging data. Consequently, the guides for both the IDIs and FGDs were dynamically modified to reflect the evolving study themes. All sessions, including IDIs and FGDs, were conducted in Kiswahili at the providers’ work premises, adding contextual depth. The IDI and FGD interview guides were originally developed in English, translated into Kiswahili (the national language), and then back translated into English to ensure that the meaning was retained. Both IDIs and FGDs were meticulously audio-recorded, transcribed verbatim, and then translated into English for analysis. Back-translation was employed to ensure validity.
Data analysis
Quantitative analysis.
Descriptive statistics are reported as frequencies and percentages or medians and interquartile ranges, with comparisons via Fisher’s exact test or the Mann‒Whitney U test as appropriate. Analyses were conducted using Stata 17.0 (Stata Corp, College Station, TX, USA).
Qualitative analysis
The analysis process, conducted concurrently with data collection, was instrumental in achieving theoretical saturation, marked by the cessation of new information from ongoing IDIs and FGDs. To ensure the validity and depth of our findings, we implemented member checking and investigator triangulation, with two independent investigators coding and interpreting the data using NVivo 2020 software (QSR International Pty Ltd., Sydney, Australia). This software facilitated a hybrid coding approach in which blended deductive and inductive methods were used for comprehensive thematic content analysis. Contextual insights from the IDIs and FGDs were key to interpreting the findings, with representative quotations included to illustrate the identified themes. Data triangulation was achieved using diverse data sources, and the research team’s expertise further enhanced the rigor and reflexivity of the analysis.
Summary of feasibility, acceptability and scalability
We used the Proctors definition of implementation outcomes and mapped the NoMAD survey results to NPT subconstructs using the definition of May et al. [ 22 , 23 ].
Feasibility is concerned with the practical aspects of implementing a new intervention, including resource allocation, training, and ease of integration into existing work. In the NPT, this aligns closely with the construct of “collective action,” which refers to the operational work that people do to enact a set of practices. To assess feasibility, we interpreted our responses as follows: “Sufficient training is provided to enable staff to use PACE” (collective action, skill set workability); “Sufficient resources are available to support PACE”; “Management adequately supports PACE” (collective action, contextual integration); and “I can easily integrate PACE into my existing work” (collective action, interactional workability).
Acceptability refers to the extent to which the new intervention is agreeable or satisfactory among its users. To assess acceptability, we interpreted our responses as follows: “Staff in this organization have a shared understanding of the purpose of PACE” (coherence: communal specification); “I believe that participating in PACE is a legitimate part of my role” (cognitive participation, legitimation); “The staff agree that PACE is worthwhile” (reflexive monitoring, communal appraisal); and “I value the effects PACE has had on my work” (reflexive monitoring, individual appraisal). In addition, we compared scores between zonal hospitals and health centers.
Scalability involves the ability to expand the intervention to other settings while maintaining its effectiveness. To assess scalability, we interpreted our responses as “I will continue to support PACE” (cognitive participation, activation); “Work is assigned to those with skills appropriate for PACE” (collective action, skill set workability); “feedback about PACE can be used to improve it in the future”; and “I can modify how I work with PACE” (reflexive monitoring, reconfiguration).
Ethical considerations
All the providers provided informed consent, and the study was approved by the Institutional Review Board of the Tanzania National Institute of Medical Research (NIMR/HO/R.8a/Vol. IX/3990), Stanford University (60379), the ethics committee of the Catholic University of Health and Allied Science (no ID number given), and the Mwanza Regional Medical Officer (Ref. No. AG.52/290/01A/115).
Techniques to enhance trustworthiness
Techniques to enhance trustworthiness included a purposeful sampling strategy, meticulous data collection in Kiswahili with back-translation, and the use of methodological, investigator, and data triangulation [ 24 ]. The analysis process was iterative and concurrent with data collection, employing hybrid coding and member checking to ensure systematic, explicit, and reproducible findings.
Reporting guidelines
This study adheres to the STROBE and SRQR reporting guidelines for comprehensive and explicit reporting of observational and qualitative studies, respectively [ 25 , 26 ].
Provider demographics
Eighty-two of the 272 eligible healthcare providers from the three facilities completed the NoMAD survey, resulting in a 30% response rate. Of the 82 respondents, 59 were from zonal hospitals and 23 from health centers (Table 2 ). The median ages were 27 and 29 years for zonal hospital and health center staff, respectively. The gender distribution was similar in both settings, with 39% female in the zonal hospital group and 43.5% in the health centers.
There were significant differences in cadre distribution: zonal hospitals had more medical staff (47.5% vs. 8.7%) and nurses (42.4% vs. 30.4%), while health centers had more clinical officers (30.4% vs. 0%). Clinical experience also varied, with a median of 1 year at zonal hospitals and 4 years at health centers ( p = 0.004). Previous participation in newborn or pediatric in-service education (e.g., Helping Babies Breathe, Helping Children Survive) was similar across the facilities, ranging from 71% to 73%. Job satisfaction scores did not significantly differ between the two groups.
A total of seventy-nine healthcare providers participated in IDIs or FGDs. Twenty-four senior providers completed IDIs, 18 from the zonal hospital and 6 from health centers., 13 FGDs with an average of 4 junior providers per group were conducted to achieve thematic saturation, including 39 participants from zonal hospitals and 16 from health centers. The represented cadres included medical officers (26, 32.9%), nurses (19, 24.1%), interns (16, 20.3%), clinical officers (12, 15.2%), assistant medical officers (3, 3.8%), and medical attendants (3, 3.8%). Clinical experience among participants ranged from 1 to 20 years. Compared to the NoMAD survey, participants in IDIs and FGDs included a higher proportion of medical officers (including interns) and clinical officers, but a lower proportion of nursing officers and other cadres.
NoMAD survey results
General items.
Familiarity and general satisfaction with PACE were high, with median scores of 89 and 91, respectively, and both showed moderate, balanced variability (interquartile ranges of 76-100 and 75-100, respectively) (Table 3 , Fig. 1 ). Optimism for the future use of PACE was highest, with a median score of 99 and narrow variability (87-100), indicating a strong skew towards higher scores. No significant differences were observed between the zonal hospitals and health centers.
NPT constructs
Providers reported understanding how to work together and plan the activities to put PACE and its components into practice. Strong agreement on the value of PACE is indicated by the median score for “Internalization" (1, “strongly agree,” IQR [1, 2]) (Table 3 , Fig. 1 ). Agreement on PACE’s purpose and its differentiation from existing work is indicated by the median scores for “Communal Specification” (2, “agree,” IQR [1, 2]), “Differentiation” (2, “agree,” IQR [1, 4]) and “Individual Specification” (2, “agree,” IQR [2, 4]), respectively. No significant differences were observed between the zonal hospitals and health centers.
Cognitive participation
Providers reported understanding how to work together to create networks of participation and communities of practice around PACE and its components. Strong agreement for ongoing PACE support, PACE participation and leadership, and PACE integration into work is indicated by the median scores for “Activation” (1, “strongly agree,” IQR [1, 1]), “Enrollment” (1, “strongly agree,” IQR [1, 1]), “Initiation” (1, “strongly agree,” IQR [1, 1]), and “Legitimation” (1, “strongly agree,” IQR [1, 2]), respectively. Narrow IQRs highlight the homogeneous support among providers. No significant differences were observed between the zonal hospitals and health centers.
Collective action
Providers reported understanding how to work together to enact PACE and its components, with greater certainty of not disrupting working relationships in the zonal hospital compared to health centers. Strong agreement that the work required by PACE is manageable, has sufficient training and resources, and receives strong organizational support is indicated by the median scores for “Interactional Workability” (1, “strongly agree,” IQR [1, 1]), “Skill-set Workability” (1, “strongly agree,” IQR [1, 2]) and “Contextual Integration” (2, “agree,” IQR [2, 2]) (Table 3 , Fig. 1 ). Agreement that PACE does not disrupt working relationships is indicated by the median score for “Relational Integration” (4, “disagree,” IQR [4, 5]). Zonal hospital providers had significantly less variability that PACE would not disrupt working relationships (relational integration)compared to health centers(IQR [4, 5] vs [3, 5] p= 0.02).
Reflexive monitoring
Providers reported understanding how to work together to evaluate the benefits of PACE and its components. Strong agreement on how people individually assess the value of PACE is indicated by the median score for “Individual Appraisal” (1, “strongly agree,” IQR [1, 1]). Agreement on how people access information to assess the value of PACE, how to value PACE collectively, and work adjustments needed for PACE is indicated by the median scores for “Systematization” (2, “agree,” IQR [2, 2]), “Communication Appraisal” (2, “agree,” IQR [2, 2]), and “Reconfiguration” (2, “agree,” IQR [2, 2]) (Table 3 , Fig. 1 ). No significant differences were observed between the zonal hospitals and health centers.
IDI and focus group results
Coherence themes.
Providers value PACE for its detailed guidance on specific pediatric cases, such as difficulty breathing, which was not covered in their basic training (Table 4 ). PACE is seen as a tool for empowering providers to reduce child mortality and improve service quality, aligning with facility goals. Providers believe that PACE has enhanced their understanding and management of seriously ill children. They find that PACE is consistent with Tanzanian and WHO guidelines and useful both in their work and in training medical students.
Cognitive participation themes
Providers were introduced to PACE by colleagues and supervisors, prompting them to enroll (Table 4 ). They mainly use PACE individually but also share modules to spread knowledge. PACE is seen as empowering providers to enhance their pediatric care. Despite busy schedules, providers are committed to PACE training.
Collective action themes
PACE's digital format allows for individual study and facilitates group discussions (Table 4 ). Initially, providers engaged with PACE for personal benefit but later saw the value in sharing knowledge. Providers value the practical application of PACE knowledge in patient care. Challenges like inadequate supplies and a lack of electricity hinder PACE implementation, but the availability of tools and support from PACE management facilitates implementation.
Reflexive monitoring themes
Providers find PACE valuable for educating junior doctors, simplifying complex topics, and boosting confidence (Table 4 ). They believe that PACE has enriched their knowledge and confidence in pediatric care. A notable challenge is the inaccessibility of learned material for future reference, hindering providers’ ability to refresh their knowledge.
Summary of feasibility, acceptability, and scalability
Overall, data from NoMAD survey responses indicated that PACE is generally feasible across healthcare settings, with providers either agreeing or strongly agreeing that people do the work required by interventions and their components (interactional workability median 1 “strongly agree” [1, 2]) or that the work of interventions and their components is supported by host organizations (contextual integration median 2 “agree” [1, 2]).
Furthermore, NoMAD survey responses indicated that PACE is also generally acceptable among healthcare providers. Providers collectively agreed about the purpose of PACE and its components (communal specification median 2 “agree” [1, 2]), agreed that PACE and its components are the right thing to do and should be part of their work (legitimation median 1 “strongly agree” [1, 2]), and collectively and individually agreed that PACE is worthwhile (communal appraisal median 2 “agree” [1, 2]; individual appraisal median 1 “strongly agree” [1, 2]).
Lastly, NoMAD survey responses indicated that PACE appears to be scalable, with some variability in its adaptability and skill-set alignment. Providers strongly agreed that they would continue to support PACE and its components (activation median 1 “strongly agree” [1, 1]), that they could modify their work in response to their appraisal of PACE, and that feedback could be used to improve it in the future (reconfiguration median 1 “strongly agree” [1, 2]). Providers agreed or were neutral about the work of PACE and its components being appropriately allocated to people (skill-set workability median 3 “neutral” [2, 4]), indicating that additional work is needed to identify the correct providers to participate in PACE or that additional support needs to be allocated to those providers to complete PACE.
This mixed-methods pilot study explored the feasibility, acceptability, and scalability of the PACE intervention among healthcare providers in Mwanza, Tanzania, using the NPT framework. The study demonstrated that PACE is generally well understood, aligns with existing healthcare goals, and is feasible to providers. There was strong acceptance and understanding that PACE should become part of normal work. Challenges to scalability lie in ensuring adequate resource and infrastructure support. Qualitative data from IDIs and FGDs enriched the findings by providing detailed insights that supported and contrasted with the NoMAD survey results, highlighting both the strengths and challenges of implementing PACE in a resource-limited setting.
Interpretation of findings
The study demonstrated that PACE is feasible. It is generally well understood by healthcare providers and aligns with existing healthcare goals. Providers found PACE to be practical in enhancing their ability to manage pediatric cases, particularly those not adequately covered in their basic training. For instance, providers appreciated the detailed guidance PACE offers for managing conditions like difficulty breathing, which they found invaluable. This alignment with healthcare objectives, such as focusing on improving service quality of newborn and child acute care to reduce child mortality underscores PACE’s potential for integration into routine clinical practice. The fact that PACE aligns with both Tanzanian and WHO guidelines further reinforces its relevance and applicability in the local healthcare context.
Provider training programs that focus on improving specific clinical performance objectives tend to yield better outcomes compared to those that cover broad topics. Targeted training programs, such as those designed to enhance specific clinical skills, have been shown to significantly improve the competency and confidence of healthcare providers. For instance, a systematic review we conducted in 2010 demonstrated that provider education programs in LMICs that focused on the needs and resources of the local healthcare environment had greater effectiveness [ 8 ]. Similarly, a study by Bluestone et al. (2013) found that focused training in neonatal resuscitation improved the performance of healthcare providers in emergency situations, as evidenced by increased neonatal survival rates [ 27 ]. In contrast, broad-topic training programs, while valuable for general knowledge enhancement, often lack the specificity needed to address critical clinical skills gaps effectively. As highlighted by Frenk et al. (2010), broad educational approaches may not adequately prepare providers for the complex, high-stakes situations they encounter in practice [ 28 ]. Therefore, training programs with a clear focus on enhancing specific clinical skills are generally more effective in improving clinical performance and patient outcomes.
The study demonstrated that PACE is acceptable. There is strong acceptance and understanding among providers that PACE should become part of their normal work. This cognitive participation reflects a high level of engagement and willingness to incorporate PACE into daily routines. Providers recognized the value of PACE in improving their knowledge and skills, with many noting that the program had significantly enhanced their understanding and management of seriously ill children. They also found PACE useful in training medical students and junior doctors, indicating its potential for broader educational impact. This widespread acceptance and integration into daily work routines suggest that PACE is viewed not just as an additional resource but as a vital component of their professional development.
When individuals perceive that a new activity should become part of their normal work, it is often associated with increased usage and integration into their daily routines [ 29 , 30 ]. This concept, known as cognitive participation, reflects a high level of engagement and commitment, which positively influences the adoption and sustained use of new practices. For instance, a study by May et al. (2009) on Normalization Process Theory highlighted that when healthcare providers viewed new clinical practices as integral to their work, they were more likely to implement them consistently [ 31 ]. Similarly, if people recognize the value of a new activity, there is substantial evidence that this recognition leads to increased usage and behavior change. Michie et al. (2011) found that perceived usefulness and perceived ease of use are significant predictors of the intention to use and actual usage of new interventions [ 32 ]. Furthermore, Rogers’ Diffusion of Innovations theory (2003) emphasizes that when individuals see clear benefits and value in a new practice, they are more likely to adopt it, leading to a transformation in their behavior and routines [ 33 ]. These findings collectively suggest that cognitive acceptance and perceived value are critical drivers of the successful implementation and sustained usage of new activities in various contexts.
However, challenges to scalability remain, particularly in ensuring adequate resource and infrastructure support. While the program itself is well-received, practical barriers such as adequate time to complete adaptive e-learning or participate in skills practice sessions and health system internet support hinder its full implementation. In addition, providers reported difficulties in accessing necessary equipment and managing cases during power outages, which directly impact their ability to apply PACE training effectively and cement long-term knowledge and skills. These challenges highlight the need for systemic improvements in resource allocation and infrastructure to support the sustainable and effective integration of PACE into the healthcare system. Without addressing these critical barriers, the scalability of PACE may be limited, preventing it from reaching its full potential impact.
Three strategies would address these challenges: 1) Strengthening Digital Infrastructure, 2) Flexible Scheduling and Time Management, and 3) Provision of Essential Equipment and Resources.
Strengthening digital infrastructure
Investing in robust digital infrastructure is crucial for the successful implementation of e-learning programs. Ensuring reliable internet connectivity and access to digital devices can significantly enhance the feasibility of adaptive learning modules. UNICEF’s conducted a review of digital learning programs in low-resource settings that highlights the positive impact of improved digital infrastructure [ 34 ]. Additionally, providing technical support and maintenance can prevent disruptions and ensure the smooth operation of online learning platforms (Aranda-Jan et al., 2014).
Flexible scheduling and time management
Allowing healthcare providers flexible scheduling to complete adaptive e-learning modules and participate in skills practice sessions can mitigate time-related barriers. Research by Yardley et al. (2012) demonstrates that flexible learning schedules increase participation and completion rates in professional development programs. Implementing self-paced learning options and modular training formats can help healthcare providers integrate training into their busy schedules without compromising clinical duties.
Provision of essential equipment and resources
Ensuring the availability of necessary medical equipment and resources is essential for the practical application of training programs. Partnerships with governmental and non-governmental organizations can facilitate the procurement and distribution of essential tools. A study by Bertram et al. (2018) suggests that strategic resource allocation and collaborative efforts can address equipment shortages and improve healthcare delivery. Additionally, creating contingency plans for managing power outages, such as providing backup power solutions, can enhance the reliability of training programs in resource-limited settings.
Qualitative data from focus groups and interviews enriched the findings by providing detailed insights that both supported and contrasted with the NoMAD survey results. These qualitative insights highlighted the strengths of PACE, such as its alignment with Tanzanian guidelines and its educational value, while also revealing challenges like resource constraints. Providers shared specific examples of how PACE had positively impacted their clinical practice, such as improving their ability to manage emergencies and enhancing their confidence in providing care. However, they also pointed out the difficulties in sustaining PACE’s benefits without adequate support and clinical resources to translate this knowledge into improved care delivery. This mixed-methods approach offered a comprehensive understanding of the implementation process, emphasizing the importance of addressing both the strengths and weaknesses of PACE in a resource-limited setting. The contrast between the high satisfaction reported in surveys and the practical challenges discussed in interviews underscores the need for a mixed methods approach when implementing new complex interventions in such environments.
Implications for implementation science and pediatric acute care
This study highlights the utility of the NPT as a conceptual framework for understanding the complexities involved in implementing adaptive learning interventions in LMICs. The findings provide valuable insights into the various factors that influence the implementation of adaptive learning, which can be applied to other healthcare interventions.
For pediatric acute care, the strong agreement among healthcare providers on the benefits of PACE for managing specific pediatric cases suggests that the program could significantly enhance provider proficiency and improve patient outcomes. Given the often time-sensitive nature of pediatric acute care, where timely and effective interventions such as oxygen therapy, intravenous fluids, and anti-microbial therapy can have a significant impact on patient outcomes, the effective and efficient training provided by PACE could lead to improved patient outcomes. Additionally, the consistency of these findings across various implementation contexts points to the scalability of the program, indicating its potential to be effectively expanded to other healthcare settings.
Limitations
The study has several limitations. The small sample size limits the generalizability of the findings, and the low response rate of 30% may introduce response bias. Additionally, the study's short duration did not allow for a comprehensive assessment of all NPT constructs, particularly reflexive monitoring. The reliance on self-reported data may also introduce social desirability bias. Our mixed methods approach, and methodological triangulation enhance the robustness of the findings despite these limitations.
Recommendations for future research
Future research should focus on longitudinal studies to assess the long-term sustainability and impact of PACE on provider proficiency, patient outcomes, and the quality of care. More rigorous qualitative research designs, such as detailed case studies and ethnographic studies, could provide a deeper understanding of the challenges and opportunities associated with implementing PACE. Additionally, research should explore the scalability of PACE, assessing how the program can be adapted for different healthcare settings and evaluating the resource implications of scaling up the intervention.
Conclusions
This study offers valuable insights into the feasibility, acceptability, and scalability of implementing PACE in a Tanzanian context. While PACE aligns well with healthcare objectives, addressing resource and infrastructure challenges is crucial for its effective and sustainable implementation. The study underscores the value of the NPT as a framework for guiding implementation processes, with broader implications for implementation science and pediatric acute care in LMICs. Future researchers can apply these insights by ensuring alignment with facility goals, engaging stakeholders early, planning for long-term evaluations, addressing resource challenges proactively, and considering the specific context and available resources when assessing scalability.
Availability of data and materials
Deidentified participant data from this study are available upon reasonable request. Interested researchers may obtain the data by contacting the corresponding author, Dr. Peter Meaney, at [email protected]. Access to the data will be granted following approval by an independent review committee established to evaluate the scientific validity and ethical justification of the proposed use of the tool. Please note that only the deidentified participant data are available, and no additional supporting information, such as study protocols or statistical analysis plans, will be provided. This process ensures that the data are used responsibly and in accordance with ethical research standards.
Data availability
Deidentified participant data from this study are available upon reasonable request. Interested researchers may obtain the data by contacting the corresponding author, Dr. Peter Meaney, at [email protected]. Access to the data will be granted following approval by an independent review committee, established to evaluate the scientific validity and ethical justification of the proposed use. Please note that only the deidentified participant data is available, and no additional supporting information, such as study protocols or statistical analysis plans, will be provided. This process ensures that the data is used responsibly and in accordance with ethical research standards.
Abbreviations
Bugando Medical Centre
Electronic Learning
Focus Group Discussion
In-Depth Interview
Low- or -Middle-Income Country
normalization process theory
normalization measure development
Pediatric Acute Care Education
Kruk ME, Gage AD, Joseph NT, Danaei G, García-Saisó S, Salomon JA. Mortality due to low-quality health systems in the universal health coverage era: a systematic analysis of amenable deaths in 137 countries. Lancet. 2018;392(10160):2203–12.
Article PubMed PubMed Central Google Scholar
Lewis TP, Roder-DeWan S, Malata A, Ndiaye Y, Kruk ME. Clinical performance among recent graduates in nine low- and middle-income countries. Trop Med Int Health. 2019;24(5):620–35.
Perin J, Mulick A, Yeung D, Villavicencio F, Lopez G, Strong KL, et al. Global, regional, and national causes of under-5 mortality in 2000–19: an updated systematic analysis with implications for the sustainable development goals. Lancet Child Adolesc Health. 2022;6(2):106–15.
Sharrow D, Hug L, Lee S, Liu Y, You D. Levels & Trends in child mortality: report 2021, estimates developed by the United Nations Inter-agency Group for Child Mortality Estimation. New York: United Nations Children’s Fund; 2021.
Google Scholar
UNICEF Data. United Republic of Tanzania (TZA) - demographics, health & infant mortality. Available from: https://data.unicef.org/country/tza/ . Cited 2023 Jun 11.
Di Giorgio L, Evans DK, Lindelow M, Nguyen SN, Svensson J, Wane W, et al. Analysis of clinical knowledge, absenteeism and availability of resources for maternal and child health: a cross-sectional quality of care study in 10 African countries. BMJ Glob Health. 2020;5(12):e003377.
Meaney PA, Sutton RM, Tsima B, Steenhoff AP, Shilkofski N, Boulet JR, et al. Training hospital providers in basic CPR skills in Botswana: acquisition, retention and impact of novel training techniques. Resuscitation. 2012;83(12):1484–90.
Meaney PA, Topjian AA, Chandler HK, Botha M, Soar J, Berg RA, et al. Resuscitation training in developing countries: a systematic review. Resuscitation. 2010;81(11):1462–72.
Article PubMed Google Scholar
Bloom BS. The 2 sigma problem: the search for methods of group instruction as effective as one-to-one tutoring. Educ Res. 1984;13(6):4–16.
Article Google Scholar
Rowe SY, Peters DH, Holloway KA, Chalker J, Ross-Degnan D, Rowe AK. A systematic review of the effectiveness of strategies to improve health care provider performance in low- and middle-income countries: methods and descriptive results. PLoS ONE. 2019;14(5):e0217617.
Article CAS PubMed PubMed Central Google Scholar
WHO. Recommendations on digital interventions for health system strengthening. World Health Organization: Geneva; 2019. Licence: CC BY-NC-SA 3.0 IGO.
Meaney PA, Hokororo A, Masenge T, Mwanga J, Kalabamu FS, Berg M, et al. Development of pediatric acute care education (PACE): an adaptive electronic learning (e-learning) environment for healthcare providers in Tanzania. Digit Health. 2023;1(9):20552076231180470.
Meaney P, Hokororo A, Ndosi H, Dahlen A, Jacob T, Mwanga JR, et al. Feasibility of an Adaptive E-Learning Environment to Improve Provider Proficiency in Essential and Sick Newborn Care in Mwanza, Tanzania. medRxiv; 2023. p. 2023.07.11.23292406. Available from: https://www.medrxiv.org/content/10.1101/2023.07.11.23292406v1 . Cited 2023 Aug 30.
Finch TL, Girling M, May CR, Mair FS, Murray E, Treweek S, et al. Improving the normalization of complex interventions: part 2 - validation of the NoMAD instrument for assessing implementation work based on normalization process theory (NPT). BMC Med Res Methodol. 2018;18(1):135.
May C, Finch T. Implementing, embedding, and integrating practices: an outline of normalization process theory. Sociology. 2009;43(3):535–54.
May C. A rational model for assessing and evaluating complex interventions in health care. BMC Health Serv Res. 2006;6(1):86.
May CR, Mair F, Finch T, MacFarlane A, Dowrick C, Treweek S, et al. Development of a theory of implementation and integration: normalization process theory. Implement Sci. 2009;4(1):29.
May CR, Cummings A, Girling M, Bracher M, Mair FS, May CM, et al. Using normalization process theory in feasibility studies and process evaluations of complex healthcare interventions: a systematic review. Implement Sci. 2018;13(1):80.
Murray E, Treweek S, Pope C, MacFarlane A, Ballini L, Dowrick C, et al. Normalisation process theory: a framework for developing, evaluating and implementing complex interventions. BMC Med. 2010;8(1):63.
McEvoy R, Ballini L, Maltoni S, O’Donnell CA, Mair FS, MacFarlane A. A qualitative systematic review of studies using the normalization process theory to research implementation processes. Implement Sci. 2014;9(1):2.
Finch TL, Rapley T, Girling M, Mair FS, Murray E, Treweek S, et al. Improving the normalization of complex interventions: measure development based on normalization process theory (NoMAD): study protocol. Implement Sci. 2013;8(1):43.
May CR, Albers B, Bracher M, Finch TL, Gilbert A, Girling M, et al. Translational framework for implementation evaluation and research: a normalisation process theory coding manual for qualitative research and instrument development. Implement Sci. 2022;17(1):19.
Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health Ment Health Serv Res. 2011;38(2):65–76.
Greenhalgh T, Taylor R. How to read a paper: papers that go beyond numbers (qualitative research). BMJ. 1997;315(7110):740–3.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–8.
O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med J Assoc Am Med Coll. 2014;89(9):1245–51.
Bluestone J, Johnson P, Fullerton J, Carr C, Alderman J, BonTempo J. Effective in-service training design and delivery: evidence from an integrative literature review. Hum Resour Health. 2013;11(1):51.
Frenk J, Chen L, Bhutta ZA, Cohen J, Crisp N, Evans T, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–58.
Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet Lond Engl. 2003;362(9391):1225–30.
Eccles MP, Grimshaw JM, MacLennan G, Bonetti D, Glidewell L, Pitts NB, et al. Explaining clinical behaviors using multiple theoretical models. Implement Sci. 2012;7(1):99.
May C, Finch T, Mair F, Ballini L, Dowrick C, Eccles M, et al. Understanding the implementation of complex interventions in health care: the normalization process model. BMC Health Serv Res. 2007;7(1):148.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci IS. 2011;23(6):42.
Rogers EM, Singhal A, Quinlan MM. Diffusion of innovations. In: An integrated approach to communication theory and research. London: Routledge; 2014. p. 432–48.
Effectiveness of digital learning solutions to improve educational outcomes | UNICEF. Available from: https://www.unicef.org/documents/effectiveness-digital-learning-solutions-improve-educational-outcomes . Cited 2024 Aug 7.
Lawrence CE, Dunkel L, McEver M, Israel T, Taylor R, Chiriboga G, et al. A REDCap-based model for electronic consent (eConsent): oving toward a more personalized consent. J Clin Transl Sci. 2020;4(4):345–53.
Download references
Acknowledgements
We are grateful to healthcare providers from Bugando Medical Centre, Makongoro and Igoma Health Centres in Mwanza City Tanzania, who participated in the study for their time, cooperation, and invaluable feedback. The authors would like to thank the Pediatric Association of Tanzania; the Tanzanian Ministry of Health, Regional and Council Health Management Teams for participating in stakeholder meetings. We thank the Catholic University of Health and Allied Sciences, London School of Hygiene and Tropical Medicine, Paediatric Association of Tanzania, and Area 9 for practical support.
REDCap database
Study data were collected and managed using REDCap electronic data capture tools hosted at Stanford University. 71,72 Research Electronic Data Capture (REDCap) is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trials for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external sources. The Stanford REDCap platform ( http://redcap.stanford.edu ) was developed and operated by the Stanford Medicine Research IT team. The REDCap platform services at Stanford are subsidized by a) the Stanford School of Medicine Research Office and b) the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through grant UL1 TR001085. Area9 Rhapsode™ meets the requirements for full GDPR compliance, including encryption, data security, and ‘forget me’.
Use of ChatGPT
We employed ChatGPT in two ways: 1) to edit and revise manuscripts for clarity to ensure adherence to writing standards (such as STROBE and SRQR) and to format manuscripts, tables, and figures; and 2) to conduct preliminary data screening/monitoring using deidentified data exported from our REDCap databases. All the statistical results and conclusions in this manuscript were confirmed by a biostatistician or member of the author group.
Patient and public involvement
This research was performed without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient-relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
1. This study was funded by the Laerdal Foundation for Acute Medicine, Stanford University School of Medicine Maternal and Child Health Research Institute, Stanford Center for Innovation in Global Health, and the Stanford University School of Medicine Division of Pediatric Critical Care Medicine.
2. Funding sources had no role in the project design; data collection, analysis, or interpretation; reporting; or decision to submit results for publication.
3. Stanford CTSA award number UL1 TR001085 from the NIH/NCRR.
Author information
Authors and affiliations.
Catholic University of Health and Allied Sciences, Mwanza, Tanzania
Joseph R. Mwanga, Adolfine Hokororo, Hanston Ndosi, Neema Chami & Enock Diocles
Pediatric Association of Tanzania, Dar Es Salaam, Tanzania
Adolfine Hokororo, Theopista Masenge, Florence S. Kalabamu, Neema Chami, Namala P. Mkopi & Castory Mwanga
Hubert Kairuki Memorial University, Dar es Salaam, Tanzania
Florence S. Kalabamu
Stanford University School of Medicine, Palo Alto, CA, USA
Daniel Tawfik, Rishi P. Mediratta, Marc Berg & Peter A. Meaney
Area9 Lyceum, Boston, MA, USA
Boris Rozenfeld
Kaiser Permanente, Oakland, CA, USA
Zachary H. Smith
Muhimbili National Hospital, Dar es Salaam, Tanzania
Namala P. Mkopi
London School of Hygiene and Tropical Medicine, London, UK
Ambrose Agweyu
You can also search for this author in PubMed Google Scholar
Contributions
R.M., A.H., H.N., and P.A.M. made substantial contributions to the conception and design of the study, as well as to the acquisition, analysis, and interpretation of data. T.M., N.C., N.P.M., and A.A. were involved in the conception and design of the study and contributed significantly to the interpretation of the data. F.S.K., M.B., and Z.S. played key roles in the conception and design of the study and contributed to data analysis. D.T., R.P.M., B.R., and C.M. were primarily responsible for data analysis and interpretation. E.D. contributed to the interpretation of data. All authors were involved in drafting the manuscript or revising it critically for important intellectual content. Each author has approved the final version to be published and agrees to be accountable for their contributions. They have also committed to ensuring that questions related to the accuracy or integrity of any part of the work, including parts in which they were not personally involved, are appropriately investigated, resolved, and documented in the literature. In accordance with the guidelines of BMC journals, we have collaborated with local colleagues where the research was conducted. They have been included as co-authors as they meet all the authorship criteria mentioned above. Contributors who did not meet all criteria for authorship are acknowledged separately. Changes to the authorship list post-submission, including any changes in the order of authors, the deletion or addition of authors, or changes in the corresponding author, will be managed according to the journal’s policy. Such changes will be finalized only upon agreement by all authors and completion of the required change of authorship form.
Author’s information
1. Joseph R. Mwanga, B.A., MSc., PhD: Senior Lecturer and Qualitative Researcher at the Catholic University of Health and Allied Sciences, Tanzania. Focuses on pediatric care and public health initiatives.
2. Adolfine Hokororo, M.D., MMed, MSc: Chief of Quality Improvement at CUHAS and Clinical Epidemiologist. Brings extensive experience in clinical quality leadership, with significant influence on healthcare policies in Tanzania through her work with NIH and USAID.
3. Hanston Ndosi, M.D.: PACE Program Manager at the Catholic University of Health and Allied Sciences, Tanzania. A crucial role is played in healthcare program management and implementation.
4. Theopista Masenge, M.D.: Vice Chair of the Pediatric Association of Tanzania and Pediatric GI Specialist. Leads implementation programs in child health and holds an MBA.
5. Florence S Kalabamu, M.D.: Pediatric Specialist at Hubert Kairuki Memorial University. Research has focused on health law and ethics.
6. Daniel Tawfik, M.D.: Assistant Professor of Pediatrics (Critical Care) at Stanford University School of Medicine. We are practicing at Stanford Medicine Children's Health, specializing in Pediatric Critical Care Medicine, and is a member of the MCHRI.
7. Rishi P Mediratta, M.D., MSc, MA: Clinical Associate Professor in Pediatrics at the Stanford University School of Medicine. A Pediatric Hospitalist at Lucile Packard Children’s Hospital and Faculty Fellow at CIGH. His work includes contributions to pediatrics and public health research in Ethiopia and teaching about the implications of COVID-19.
8. Boris Rozenfeld, M.D.: Learning Architect for Healthcare Education at Area9 Lyceum. Leads a team of medical learning engineers with a strong background in CME and educational technology.
9. Marc Berg, M.D.: Clinical Professor in Pediatrics - Critical Care at Stanford University School of Medicine. Her research interests included CPR performance and pediatric defibrillation science through simulation. Medical Director of the Revive Initiative for Pediatric Resuscitation Excellence.
10. Zack Haines Smith, M.D., M.P.H.: Pediatric Critical Care Physician at Kaiser Permanente, Oakland, CA.
11. Neema Chami, M.D.: Neonatologist at Bugando Medical Center, Pediatric Faculty at CUHAS, Subject Matter Expert and Learning Engineer for PACE, and Key Member of the Pediatric Association of Tanzania.
12. Namala P Mkopi, M.D.: Tanzania’s first Pediatric Critical Care Physician, leading Pediatric Critical Care at Muhimbili National Hospital and Subject Matter Expert and Learning Engineer for PACE.
13. Castory Mwanga, M.D.: Senior Pediatrician and Leader at Simiyu Designated District Hospital, Subject Matter Expert and Learning Engineer for PACE, focusing on pediatric healthcare services.
14. Enock Diocles, M.D.: Nurse Educator at Mwanza College of Allied Sciences, Researcher, Clinician, and Founding Member of the Tanzanian Pediatric Nursing Association.
15. Ambrose Agweyu, M.D., MSc.: Kenyan Pediatrician and Professor of Epidemiology at the London School of Hygiene and Tropical Medicine. Influential in adapting WHO guidelines for Kenya and leading clinical trials for childhood pneumonia treatment.
16. Peter Andrew Meaney, M.D., MPH: Clinical Professor at Stanford University School of Medicine specializing in Pediatric Critical Care Medicine. His research focuses on provider education, implementation science, and quality care in resource-limited settings. He is an Associate Program Director for the T-32 Pediatric Subspecialty Global Health Fellowship and a Global Health Faculty Fellow at CIGH.
Corresponding author
Correspondence to Peter A. Meaney .
Ethics declarations
Ethics approval and consent to participate.
The Institutional Review Board of the Tanzania National Institute of Medical Research (NIMR/HO/R.8a/Vol. IX/3990), Stanford University (60379), the ethics committee of the Catholic University of Health and Allied Science (no ID number given), and the Mwanza Regional Medical Officer (Ref. No. AG.52/290/01A/115) approved the study protocol, including consent. The data collection procedures were completed in compliance with the guidelines of the Health Insurance Portability and Accountability Act (HIPAA) to ensure subject confidentiality. Informed electronic consent was obtained through REDCap from all providers who participated in the PACE [ 35 ]. All providers who provided consent were included. All the surveys and questionnaires were entered directly by providers into REDCap. This study is reported according to the Consolidated Standards of Reporting Trials (CONSORT) 2010 extension to randomized pilot and feasibility trials.
Consent for publication
All individual persons’ data included in this study are entirely unidentifiable, and there are no details on individuals reported within the manuscript. Therefore, consent for publication is not applicable to this study. If there were any identifiable details, images, or videos relating to individual persons, consent would be obtained from those persons or, in the case of children, their parent or legal guardian as noted in this section accordingly.
Competing interests
BR and MB are compensated by Area 9 Lyceum as Senior Learning Architect and Medical Director, respectively.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Mwanga, J.R., Hokororo, A., Ndosi, H. et al. Evaluating the implementation of the Pediatric Acute Care Education (PACE) program in northwestern Tanzania: a mixed-methods study guided by normalization process theory. BMC Health Serv Res 24 , 1066 (2024). https://doi.org/10.1186/s12913-024-11554-3
Download citation
Received : 16 May 2024
Accepted : 06 September 2024
Published : 13 September 2024
DOI : https://doi.org/10.1186/s12913-024-11554-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Adaptive learning
- Feasibility
- Acceptability
- Normalization Process Theory
- Implementation Science
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]
IMAGES
VIDEO
COMMENTS
A case study is one of the most commonly used methodologies of social research. This article attempts to look into the various dimensions of a case study research strategy, the different epistemological strands which determine the particular case study type and approach adopted in the field, discusses the factors which can enhance the effectiveness of a case study research, and the debate ...
Defnition: A case study is a research method that involves an in-depth examination and analysis of a particular phenomenon or case, such as an individual, organization, community, event, or situation. It is a qualitative research approach that aims to provide a detailed and comprehensive understanding of the case being studied.
the studies. Exploring a life is different from generating a theory or describing the behavior of a cultural group. A couple of potential similarities among the designs should be noted. Narrative research, ethnography, and case study research may seem similar when the unit of analysis is a single individual. True, one may approach
There are at least three primary applications of theory in qualitative research: (1) theory of research paradigm and method (Glesne, 2011), (2) theory building as a result of data collection (Jaccard & Jacoby, 2010), and (3) theory as a framework to guide the study (Anfara & Mertz, 2015). Differentiation and clarification between these ...
In qualitative research, case study is one of the frequently used methodologies (Yazan, 2015). ... Critical theory research suggests that reality is historically established, and it is produced and reproduced by people (Meyers, 2004). Critical studies seek to expose contradictions and flaws in social systems with a view to make some sort of ...
A case study is a detailed study of a specific subject, such as a person, group, place, event, organization, or phenomenon. Case studies are commonly used in social, educational, clinical, and business research. A case study research design usually involves qualitative methods, but quantitative methods are sometimes also used.
A case study is a research approach that is used to generate an in-depth, multi-faceted understanding of a complex issue in its real-life context. It is an established research design that is used extensively in a wide variety of disciplines, particularly in the social sciences. A case study can be defined in a variety of ways (Table 5), the ...
The purpose of case study research is twofold: (1) to provide descriptive information and (2) to suggest theoretical relevance. Rich description enables an in-depth or sharpened understanding of the case. It is unique given one characteristic: case studies draw from more than one data source. Case studies are inherently multimodal or mixed ...
Definitions of qualitative case study research. Case study research is an investigation and analysis of a single or collective case, intended to capture the complexity of the object of study (Stake, 1995).Qualitative case study research, as described by Stake (), draws together "naturalistic, holistic, ethnographic, phenomenological, and biographic research methods" in a bricoleur design ...
Abstract. This chapter explores case study as a major approach to research and evaluation. After first noting various contexts in which case studies are commonly used, the chapter focuses on case study research directly Strengths and potential problematic issues are outlined and then key phases of the process.
Introduction. The popularity of case study research methodology in Health Services Research (HSR) has grown over the past 40 years. 1 This may be attributed to a shift towards the use of implementation research and a newfound appreciation of contextual factors affecting the uptake of evidence-based interventions within diverse settings. 2 Incorporating context-specific information on the ...
McMaster University, West Hamilton, Ontario, Canada. Qualitative case study methodology prov ides tools for researchers to study. complex phenomena within their contexts. When the approach is ...
Abstract. This article presents the case study as a type of qualitative research. Its aim is to give a detailed description of a case study - its definition, some classifications, and several ...
The major types of qualitative research designs are narrative research, phenomenological research, grounded theory research, ethnographic research, historical research, and case study research. The greatest strength of the qualitative research approach lies in the richness and depth of the healthcare exploration and description it makes.
Summary. The chapter re-examines the case study research method and its role and contribution to the IS discipline and focuses on the current status of the case study research and the increased digitalization. The advantages of qualitative interpretive cases studies are identified, recent case studies are described and analyzed, and their ...
This paper, drawing from the literature, discusses the philosophical position of case study research and argues that qualitative case study research is appropriate for theory. building. For theory ...
2.1 Case study research design 1: no theory first. A popular template for building theory from case studies is a paper by Eisenhardt (1989). It follows a dramaturgy with a precise order of single steps for constructing a case study and is one of the most cited papers in methods sections (Ravenswood 2011).
While many books and articles guide various qualitative research methods and analyses, there is currently no concise resource that explains and differentiates among the most common qualitative approaches. We believe novice qualitative researchers, students planning the design of a qualitative study or taking an introductory qualitative research course, and faculty teaching such courses can ...
Once a theory is developed from qualitative studies, a quantitative researcher can seek to test that theory. ... In that case, the researcher would ... they can change over the course of a study. Qualitative research is a reflexive process, one in which the researcher adapts their approach based on what participants say and do. The researcher ...
Thomas argues that the terms "theory" and "induction" are not appropriate for the specificity of the insights that case studies generate and should be replaced by "abduction" and "phronesis" (Thomas, 2010).We argue that theory, despite its limitations in the social sciences, is an important and necessary aspect of case study research.
Qualitative research is an advanced field of study. The key aim of this chapter was to discuss the three major types of qualitative research—narrative inquiry, phenomenology, and grounded theory. This chapter firstly provided a brief discussion on qualitative research, its philosophical foundations, and types. Secondly, it provided a ...
This collection brings together researchers and scholars from across the Arts, Humanities and Social Sciences who are actively exploring the many different ways in which time might be understood, imagined and used in qualitative research. Taken together, the contributions begin to trace the contours of what it might mean to work reflexively ...
SAGE Research Methods links over 175,000 pages of SAGE's renowned book, journal and reference content with truly advanced search and discovery tools. Researchers can explore methods concepts to help them design research projects, understand particular methods or identify a new method, conduct their research, and write up their findings.
A Study of Faculty Acceptance of a Faculty Information Survey (1974) John Ward Creswell is an American academician known for his work in mixed methods research . He has written numerous journal articles and 27 books on mixed methods research, research methods , and qualitative research .
The qualitative study was reported following the Consolidated Criteria for Reporting Qualitative Research checklist . Participants. Considering that academic and clinical nurses were the main stakeholders in APPs-EBN course for undergraduate nursing students, this study conducted qualitative interviews with these two groups of people.
Temporal theory: preparedness across healthcare professions through and over time. Time is central to qualitative longitudinal research (QLR: Neale, 2018, 2019), and can be conceptualised in various ways (Rees & Ottrey, in press).In health-related QLR, time is often conceptualised as change, process, transition, and development (Audulv et al., 2022).
The case study approach to research is a way of conducting mainly qualitative inquiry, commonly used when it is impossible to control all of the variables that are of interest to the researcher.
This qualitative, single case study examined Black graduate students' perceptions of a university president's responses to racialized incidents and how these perceptions inform Black graduate students' larger contextual understanding of campus racial climate. Guided by Hurtado et al.'s (2012) Multi-Contextual Model for Diverse Learning Environments, the research questions were: What ...
More rigorous qualitative research designs, such as detailed case studies and ethnographic studies, could provide a deeper understanding of the challenges and opportunities associated with implementing PACE. ... MacFarlane A. A qualitative systematic review of studies using the normalization process theory to research implementation processes ...
Ever since family systems therapy became a field of study in the mid‐20th century, family functioning has defied numeric data, making families about as easy to measure as the quantum world, with all their complexity and variability - and messiness. Over the years, numerous quantitative measures have attempted to master this feat, with varying success. However, quantitative, postpositivist ...